Olbet AM 20 Tablet









Therapy Area
Cardiology
1.0 Generic name
Amlodipine and Olmesartan Medoxomil Tablets IP
2.0 Qualitative and quantitative composition
Olbet AM 20
Each film-coated tablet contains:
Amlodipine Besilate IP equivalent to Amlodipine 5 mg
Olmesartan Medoxomil IP 20 mg
Excipients q.s.
Colours: Lake of Quinoline Yellow WS & Titanium Dioxide IP
Olbet-AM 40
Each film-coated tablet contains:
Amlodipine Besilate IP equivalent to Amlodipine 5 mg
Olmesartan Medoxomil IP 40 mg
Excipients q.s.
Colours: Lake of Quinoline Yellow WS & Titanium Dioxide IP
3.0 Dosage form and strength
Film-coated tablet.
5mg/20mg and 5mg/40mg
4.0 Clinical particulars
4.1 Therapeutic Indications
Olbet AM 20:
- For the treatment of mild to moderate hypertension.
Olbet-AM 40:
- For the treatment of hypertension alone or with other antihypertensive agents
- To use as initial therapy in patients who are likely to need multiple antihypertensive agents to achieve their blood pressure goals.
4.2 Posology and Method of Administration
Adults
The recommended dosage of Olbet-AM is one tablet per day.
Olbet-AM 5 mg/20 mg may be administered in patients whose blood pressure is not adequately controlled by 20 mg olmesartan medoxomil or 5 mg amlodipine alone.
Olbet-AM 5 mg/ 40 mg may be administered in patients whose blood pressure is not adequately controlled by Olbet-AM 20 mg/5 mg.
A stepwise titration of the dosage of the individual components is recommended before changing to the fixed combination. When clinically appropriate, direct change from monotherapy to the fixed combination may be considered. For convenience, patients receiving olmesartan medoxomil and amlodipine from separate tablets may be switched to Olbet-AM tablets containing the same component doses. Olbet-AM can be taken with or without food.
Older people (age 65 years or over)
No adjustment of the recommended dose is generally required for older people but increase of the dosage should take place with care. Blood pressure should be closely monitored If up titration to the maximum dose of 40 mg olmesartan daily is required.
Renal impairment
The maximum dose of olmesartan medoxomil in patients with mild to moderate renal impairment (creatinine clearance of 20 – 60 mL/min) is 20 mg olmesartan medoxomil once daily, owing to limited experience of higher dosages in this patient group. The use of Olbet-AM in patients with severe renal impairment (creatinine clearance < 20 mL/min) is not recommended. Monitoring of potassium levels and creatinine is advised in patients with moderate renal impairment.
Hepatic impairment
Olbet-AM should be used with caution in patients with mild to moderate hepatic impairment. In patients with moderate hepatic impairment, an initial dose of 10 mg olmesartan medoxomil once daily is recommended and the maximum dose should not exceed 20 mg once daily. As with all calcium antagonists, amlodipine's half life is prolonged in patients with impaired liver function and dosage recommendations have not been established. Olbet-AM should therefore be administered with caution in these patients. Use of Olbet-AM in patients with severe hepatic impairment is contraindicated.
Paediatric population
The safety and efficacy of Olbet-AM in children and adolescents below 18 years has not been established.
Method of administration
The tablet should be swallowed with a sufficient amount of fluid (e.g. one glass of water). The tablet should not be chewed and should be taken at the same time each day.
4.3 Contraindications
- Hypersensitivity to the active substances, to dihydropyridine derivatives or to any of the excipients
- Second and third trimesters of pregnancy.
- Severe hepatic insufficiency and biliary obstruction.
- The concomitant use of Olbet-AM with aliskiren containing products is contraindicated in patients with diabetes mellitus or renal impairment (GFR < 60 mL/min/1.73 m2).
Due to the component amlodipine, Olbet-AM is also contraindicated in patients with:
- Severe hypotension.
- Shock (including cardiogenic shock).
- Obstruction of the outflow tract of the left ventricle (e.g. aortic stenosis).
- Hemodynamically unstable heart failure after acute myocardial infarction
4.4 Special Warnings and Precautions for Use
Patients with hypovolaemia or sodium depletion:
Symptomatic hypotension may occur in patients who are volume and/or sodium depleted by vigorous diuretic therapy, dietary salt restriction, and diarrhoea or vomiting, especially after the first dose. Correction of this condition prior to administration of Olbet-AM or close medical supervision at the start of the treatment is recommended.
Other conditions with stimulation of the renin-angiotensin-aldosterone system:
In patients whose vascular tone and renal function depend predominantly on the activity of the renin-angiotensin-aldosterone system (e.g. patients with severe congestive heart failure or underlying renal disease, including renal artery stenosis), treatment with other medicinal products that affect this system, such as angiotensin II receptor antagonists, has been associated with acute hypotension, azotaemia, oliguria or, rarely, acute renal failure.
Renovascular hypertension:
There is an increased risk of severe hypotension and renal insufficiency when patients with bilateral renal artery stenosis or stenosis of the artery to a single functioning kidney are treated with medicinal products that affect the renin-angiotensin-aldosterone system.
Renal impairment and kidney transplantation:
When Olbet-AM is used in patients with impaired renal function, periodic monitoring of serum potassium and creatinine levels is recommended. Use of Olbet-AM is not recommended in patients with severe renal impairment (creatinine clearance < 20 mL/min). There is no experience of the administration of Olbet-AM in patients with a recent kidney transplant or in patients with end-stage renal impairment (i.e. creatinine clearance < 12 mL/min).
Dual blockade of the renin-angiotensin-aldosterone system (RAAS):
There is evidence that the concomitant use of ACE-inhibitors, angiotensin II receptor blockers or aliskiren increases the risk of hypotension, hyperkalaemia and decreased renal function (including acute renal failure). Dual blockade of RAAS through the combined use of ACE-inhibitors, angiotensin II receptor blockers or aliskiren is therefore not recommended.
If dual blockade therapy is considered necessary, this should only occur under specialist supervision and subject to frequent close monitoring of renal function, electrolytes and blood pressure.
ACE-inhibitors and angiotensin II receptor blockers should not be used concomitantly in patients with diabetic nephropathy.
Hepatic impairment:
Exposure to amlodipine and olmesartan medoxomil is increased in patients with hepatic impairment. Care should be taken when Olbet-AM is administered in patients with mild to moderate hepatic impairment. In moderately impaired patients, the dose of olmesartan medoxomil should not exceed 20 mg. In patients with impaired hepatic function, amlodipine should be initiated at the lower end of the dosing range and caution should be used, both on initial treatment and when increasing the dose. Use of Olbet-AM in patients with severe hepatic impairment is contraindicated.
Hyperkalaemia:
As with other angiotensin II antagonists and ACE inhibitors, hyperkalaemia may occur during treatment, especially in the presence of renal impairment and/or heart failure. Close monitoring of serum potassium levels in at-risk patients is recommended.
Concomitant use with potassium supplements, potassium-sparing diuretics, salt substitutes containing potassium, or other medicinal products that may increase potassium levels (heparin, etc.) should be undertaken with caution and with frequent monitoring of potassium levels.
Lithium:
As with other angiotensin II receptor antagonists, the concomitant use of Olbet-AM and lithium is not recommended.
Aortic or mitral valve stenosis; obstructive hypertrophic cardiomyopathy:
Due to the amlodipine component of Olbet-AM, as with all other vasodilators, special caution is indicated in patients suffering from aortic or mitral valve stenosis, or obstructive hypertrophic cardiomyopathy.
Primary aldosteronism:
Patients with primary aldosteronism generally will not respond to antihypertensive medicinal products acting through inhibition of the renin-angiotensin system. Therefore, the use of Olbet-AM is not recommended in such patients.
Heart failure:
As a consequence of the inhibition of the renin-angiotensin-aldosterone system, changes in renal function may be anticipated in susceptible individuals. In patients with severe heart failure whose renal function may depend on the activity of the renin-angiotensin-aldosterone system, treatment with angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor antagonists has been associated with oliguria and/or progressive azotaemia and (rarely) with acute renal failure and/or death.
Patients with heart failure should be treated with caution. In a long-term, placebo controlled study of amlodipine in patients with severe heart failure (NYHA III and IV), the reported incidence of pulmonary oedema was higher in the amlodipine group than in the placebo group. Calcium channel blockers, including amlodipine, should be used with caution in patients with congestive heart failure, as they may increase the risk of future cardiovascular events and mortality.
Sprue-like enteropathy:
In very rare cases severe, chronic diarrhoea with substantial weight loss has been reported in patients taking olmesartan few months to years after drug initiation, possibly caused by a localized delayed hypersensitivity reaction. Intestinal biopsies of patients often demonstrated villous atrophy. If a patient develops these symptoms during treatment with olmesartan, and in the absence of other apparent etiologies, olmesartan treatment should be immediately discontinued and should not be restarted. If diarrhoea does not improve during the week after the discontinuation, further specialist (e.g. a gastro-enterologist) advice should be considered.
Ethnic differences:
As with all other angiotensin II antagonists, the blood pressure lowering effect of Olbet-AM can be somewhat less in black patients than in non-black patients, possibly because of a higher prevalence of low-renin status in the black hypertensive population.
Elderly
In the elderly, increase of the dosage should take place with care.
Pregnancy:
Angiotensin II antagonists should not be initiated during pregnancy. Unless continued angiotensin II antagonist therapy is considered essential, patients planning pregnancy should be changed to alternative antihypertensive treatments which have an established safety profile for use in pregnancy. When pregnancy is diagnosed, treatment with angiotensin II antagonists should be stopped immediately, and, if appropriate, alternative therapy should be started.
Other:
As with any antihypertensive agent, excessive blood pressure decrease in patients with ischaemic heart disease or ischaemic cerebrovascular disease could result in a myocardial infarction or stroke.
4.5 Drugs interactions
Potential interactions related to the Olbet-AM combination:
To be taken into account with concomitant use
Other antihypertensive agents:
The blood pressure lowering effect of Olbet-AM can be increased by concomitant use of other antihypertensive medicinal products (e.g. alpha-blockers, diuretics).
Potential interactions related to the olmesartan medoxomil component of Olbet-AM:
Concomitant use not recommended
ACE-inhibitors, angiotensin II receptor blockers or aliskiren:
Clinical trial data has shown that dual blockade of the renin-angiotensin-aldosterone-system (RAAS) through the combined use of ACE-inhibitors, angiotensin II receptor blockers or aliskiren is associated with a higher frequency of adverse events such as hypotension, hyperkalaemia and decreased renal function (including acute renal failure) compared to the use of a single RAAS-acting agent.
Medicinal products affecting potassium levels:
Concomitant use of potassium-sparing diuretics, potassium supplements, salt substitutes containing potassium or other medicinal products that may increase serum potassium levels (e.g. heparin, ACE inhibitors) may lead to increases in serum potassium. If medicinal products, which affect potassium levels, are to be prescribed in combination with Olbet-AM, monitoring of serum potassium levels is recommended.
Lithium:
Reversible increases in serum lithium concentrations and toxicity have been reported during concomitant administration of lithium with angiotensin converting enzyme inhibitors and, rarely, with angiotensin II antagonists. Therefore, concomitant use of Olbet-AM and lithium is not recommended. If concomitant use of Olbet-AM and lithium proves necessary, careful monitoring of serum lithium levels is recommended.
Concomitant use requiring caution
Non-steroidal anti-inflammatory medicinal products (NSAIDs) including selective COX-2 inhibitors, acetylsalicylic acid (> 3 g/day) and non-selective NSAIDs:
When angiotensin II antagonists are administered simultaneously with NSAIDs, attenuation of the antihypertensive effect may occur. Furthermore, concomitant use of angiotensin II antagonists and NSAIDs may increase the risk of worsening of renal function and may lead to an increase in serum potassium. Therefore monitoring of renal function at the beginning of such concomitant therapy is recommended, as well as adequate hydration of the patient.
Bile acid sequestering agent colesevelam:
Concurrent administration of the bile acid sequestering agent colesevelam hydrochloride reduces the systemic exposure and peak plasma concentration of olmesartan and reduces t1/2. Administration of olmesartan medoxomil at least 4 hours prior to colesevelam hydrochloride decreased the drug interaction effect. Administering olmesartan medoxomil at least 4 hours before the colesevelam hydrochloride dose should be considered.
Additional information
After treatment with antacid (aluminium magnesium hydroxide), a modest reduction in bioavailability of olmesartan was observed.
Olmesartan medoxomil had no significant effect on the pharmacokinetics or pharmacodynamics of warfarin or the pharmacokinetics of digoxin. Coadministration of olmesartan medoxomil with pravastatin had no clinically relevant effects on the pharmacokinetics of either component in healthy subjects.
Olmesartan had no clinically relevant inhibitory effects on human cytochrome P450 enzymes 1A1/2, 2A6, 2C8/9, 2C19, 2D6, 2E1 and 3A4 in vitro, and had no or minimal inducing effects on rat cytochrome P450 activities. No clinically relevant interactions between olmesartan and medicinal products metabolised by the above cytochrome P450 enzymes are expected.
Potential interactions related to the amlodipine component of Olbet-AM:
Effects of other medicinal products on amlodipine
CYP3A4 inhibitors:
Concomitant use of amlodipine with strong or moderate CYP3A4 inhibitors (protease inhibitors, azole antifungals, macrolides like erythromycin or clarithromycin, verapamil or diltiazem) may give rise to significant increase in amlodipine exposure. The clinical translation of these PK variations may be more pronounced in the elderly. There is an increased risk of hypotension. Close observation of patients is recommended and dose adjustment may thus be required.
CYP3A4 inducers:
Upon co-administration of known inducers of the CYP3A4, the plasma concentration of amlodipine may vary. Therefore, blood pressure should be monitored and dose regulation considered both during and after concomitant medication particularly with strong CYP3A4 inducers (e.g. rifampicin, hypericum perforatum).
Administration of amlodipine with grapefruit or grapefruit juice is not recommended as bioavailability may be increased in some patients resulting in increased blood pressure lowering effects.
Dantrolene (infusion): In animals, lethal ventricular fibrillation and cardiovascular collapse are observed in association with hyperkalaemia after administration of verapamil and intravenous dantrolene. Due to risk of hyperkalaemia, it is recommended that the co-administration of calcium channel blockers such as amlodipine be avoided in patients susceptible to malignant hyperthermia and in the management of malignant hyperthermia.
Effects of amlodipine on other medicinal products
The blood pressure lowering effects of amlodipine adds to the blood pressure-lowering effects of other antihypertensive agents.
In clinical interaction studies, amlodipine did not affect the pharmacokinetics of atorvastatin, digoxin or warfarin.
Simvastatin: Co-administration of multiple doses of 10 mg of amlodipine with 80 mg simvastatin resulted in a 77% increase in exposure to simvastatin compared to simvastatin alone. Limit the dose of simvastatin in patients on amlodipine to 20 mg daily.
Tacrolimus: There is a risk of increased tacrolimus blood levels when co-administered with amlodipine. In order to avoid toxicity of tacrolimus, administration of amlodipine in a patient treated with tacrolimus requires monitoring of tacrolimus blood levels and dose adjustment of tacrolimus when appropriate.
Mechanistic Target of Rapamycin (mTOR) Inhibitors: mTOR inhibitors such as sirolimus, temsirolimus, and everolimus are CYP3A substrates. Amlodipine is a weak CYP3A inhibitor. With concomitant use of mTOR inhibitors, amlodipine may increase exposure of mTOR inhibitors.
Cyclosporine: In a prospective study in renal transplant patients, an average 40% increase in trough cyclosporine levels was observed when used concomitantly with amlodipine. The co-administration of Olbet-AM with cyclosporine may increase exposure to cyclosporine. Monitor trough cyclosporine levels during concomitant use and cyclosporine dose reductions should be made as necessary.
4.6 Use in special populations
Pregnancy
There are no data about the use of Olbet-AM in pregnant patients. Animal reproductive toxicity studies with Olbet-AM have not been performed.
Olmesartan medoxomil
The use of angiotensin II antagonists is not recommended during the first trimester of pregnancy. The use of angiotensin II antagonists is contraindicated during the 2nd and 3rd trimesters of pregnancy.
Epidemiological evidence regarding the risk of teratogenicity following exposure to ACE inhibitors during the first trimester of pregnancy has not been conclusive; however a small increase in risk cannot be excluded. Whilst there is no controlled epidemiological data on the risk with angiotensin II antagonists, similar risks may exist for this class of drugs. Unless continued angiotensin II antagonists therapy is considered essential, patients planning pregnancy should be changed to alternative anti-hypertensive treatments which have an established safety profile for use in pregnancy. When pregnancy is diagnosed, treatment with angiotensin II antagonists should be stopped immediately, and, if appropriate, alternative therapy should be started.
Exposure to angiotensin II antagonists therapy during the second and third trimesters is known to induce human fetotoxicity (decreased renal function, oligohydramnios, skull ossification retardation) and neonatal toxicity (renal failure, hypotension, hyperkalaemia).
Should exposure to angiotensin II antagonists have occurred from the second trimester on, ultrasound check of renal function and skull is recommended. Infants whose mothers have taken angiotensin II antagonists should be closely observed for hypotension.
Amlodipine
Data on a limited number of exposed pregnancies do not indicate that amlodipine or other calcium receptor antagonists have a harmful effect on the health of the fetus. However, there may be a risk of prolonged delivery.
Therefore, Olbet-AM is not recommended during the first trimester of pregnancy and is contraindicated during the second and third trimesters of pregnancy.
Breastfeeding
Olmesartan is excreted into the milk of lactating rats. However, it is not known whether olmesartan passes into human milk.
Amlodipine is excreted in human milk. The proportion of the maternal dose received by the infant has been estimated with an interquartile range of 3 – 7%, with a maximum of 15%. The effect of amlodipine on infants is unknown.
During breast-feeding, Olbet-AM is not recommended and alternative treatments with better-established safety profiles during breast-feeding are preferable, especially while nursing a newborn or preterm infant.
4.7 Effects on Ability to Drive and Use Machines
Olbet-AM can have minor or moderate influence on the ability to drive and use machines.
Dizziness, headache, nausea or fatigue may occasionally occur in patients taking antihypertensive therapy, which may impair the ability to react. Caution is recommended especially at the start of treatment.
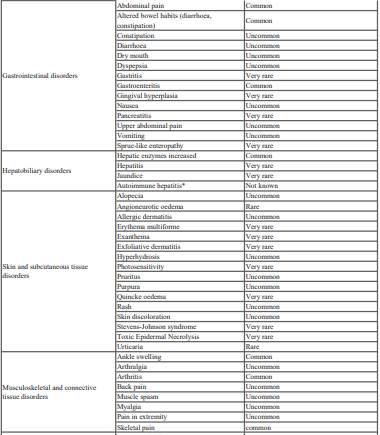
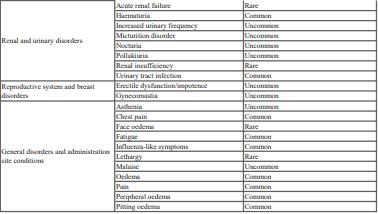
4.8 Undesirable Effects
The most commonly reported adverse reactions during treatment with Olbet AM are peripheral oedema (11.3%), headache (5.3%) and dizziness (4.5%).
The following terminologies have been used in order to classify the occurrence of adverse reactions: Very common (≥ 1/10), Common (≥ 1/100 to <1/10), Uncommon (≥ 1/1,000 to <1/100), Rare (≥ 1/10,000 to <1/1,000), Very rare (<1/10,000), not known (cannot be estimated from the available data)

Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via email to: medico@zuventus.com
Website: https://www.zuventus.com/drug-safety-reporting
4.9 Overdose
Symptoms:
There is no experience of overdose with Olbet-AM. The most likely effects of olmesartan medoxomil overdosage are hypotension and tachycardia; bradycardia could be encountered if parasympathetic (vagal) stimulation occurred. Amlodipine overdosage can be expected to lead to excessive peripheral vasodilatation with marked hypotension and possibly a reflex tachycardia. Marked and potentially prolonged systemic hypotension up to and including shock with fatal outcome has been reported.
Non-cardiogenic pulmonary oedema has rarely been reported as a consequence of amlodipine overdose that may manifest with a delayed onset (24-48 hours post-ingestion) and require ventilatory support. Early resuscitative measures (including fluid overload) to maintain perfusion and cardiac output may be precipitating factors.
Treatment:
If intake is recent, gastric lavage may be considered. In healthy subjects, the administration of activated charcoal immediately or up to 2 hours after ingestion of amlodipine has been shown to reduce substantially the absorption of amlodipine.
Clinically significant hypotension due to an overdose of Olbet-AM requires active support of the cardiovascular system, including close monitoring of heart and lung function, elevation of the extremities, and attention to circulating fluid volume and urine output. A vasoconstrictor may be helpful in restoring vascular tone and blood pressure, provided that there is no contraindication to its use. Intravenous calcium gluconate may be beneficial in reversing the effects of calcium channel blockade.
Since amlodipine is highly protein-bound, dialysis is not likely to be of benefit. The dialysability of olmesartan is unknown.
5.0 Pharmacological properties
5.1 Pharmacodynamic Properties
Pharmacotherapeutic group: Angiotensin II antagonists and calcium channel blockers, ATC code C09DB02.
Mechanism of action
Olbet-AM is a combination of an angiotensin II receptor antagonist, olmesartan medoxomil, and a calcium channel blocker, amlodipine besilate. The combination of these active ingredients has an additive antihypertensive effect, reducing blood pressure to a greater degree than either component alone.
The antihypertensive effect of Olbet-AM was similar irrespective of age and gender, and was similar in patients with and without diabetes.
Olmesartan medoxomil
The olmesartan medoxomil component of Olbet-AM is a selective angiotensin II type 1 (AT1) receptor antagonist. Olmesartan medoxomil is rapidly converted to the pharmacologically active metabolite, olmesartan. Angiotensin II is the primary vasoactive hormone of the renin-angiotensin-aldosterone system and plays a significant role in the pathophysiology of hypertension. The effects of angiotensin II include vasoconstriction, stimulation of the synthesis and release of aldosterone, cardiac stimulation and renal reabsorption of sodium. Olmesartan blocks the vasoconstrictor and aldosterone-secreting effects of angiotensin II by blocking its binding to the AT1 receptor in tissues including vascular smooth muscle and the adrenal gland. The action of olmesartan is independent of the source or route of synthesis of angiotensin II. The selective antagonism of the angiotensin II (AT1) receptors by olmesartan results in increases in plasma renin levels and angiotensin I and II concentrations, and some decrease in plasma aldosterone concentrations.
In hypertension, olmesartan medoxomil causes a dose-dependent, long-lasting reduction in arterial blood pressure. There has been no evidence of first-dose hypotension, of tachyphylaxis during long-term treatment, or of rebound hypertension after abrupt cessation of therapy.
Following once daily administration to patients with hypertension, olmesartan medoxomil produces an effective and smooth reduction in blood pressure over the 24 hour dose interval. Once daily dosing produced similar decreases in blood pressure as twice daily dosing at the same total daily dose.
With continuous treatment, maximum reductions in blood pressure are achieved by 8 weeks after the initiation of therapy, although a substantial proportion of the blood pressure lowering effect is already observed after 2 weeks of treatment.
The effect of olmesartan medoxomil on mortality and morbidity is not yet known.
Amlodipine
The amlodipine component of Olbet-AM is a calcium channel blocker that inhibits the transmembrane influx of calcium ions through the potential-dependent L-type channels into the heart and smooth muscle. Experimental data indicate that amlodipine binds to both dihydropyridine and non-dihydropyridine binding sites. Amlodipine is relatively vessel-selective, with a greater effect on vascular smooth muscle cells than on cardiac muscle cells. The antihypertensive effect of amlodipine derives from a direct relaxant effect on arterial smooth muscle, which leads to a lowering of peripheral resistance and hence of blood pressure.
In hypertensive patients, amlodipine causes a dose-dependent, long-lasting reduction in arterial blood pressure. There has been no evidence of first-dose hypotension, of tachyphylaxis during long-term treatment, or of rebound hypertension after abrupt cessation of therapy.
Following administration of therapeutic doses to patients with hypertension, amlodipine produces an effective reduction in blood pressure in the supine, sitting and standing positions. Chronic use of amlodipine is not associated with significant changes in heart rate or plasma catecholamine levels. In hypertensive patients with normal renal function, therapeutic doses of amlodipine reduce renal vascular resistance and increase glomerular filtration rate and effective renal plasma flow, without changing filtration fraction or proteinuria.
In haemodynamic studies in patients with heart failure and in clinical studies based on exercise tests in patients with NYHA class II-IV heart failure, amlodipine was found not to cause any clinical deterioration, as measured by exercise tolerance, left ventricular ejection fraction and clinical signs and symptoms.
5.2 Pharmacokinetic Properties
Olbet-AM
Following oral intake of Olbet-AM, peak plasma concentrations of olmesartan and amlodipine are reached at 1.5 – 2 h and 6 – 8 hours, respectively. The rate and extent of absorption of the two active substances from Olbet-AM are equivalent to the rate and extent of absorption following intake of the two components as separate tablets. Food does not affect the bioavailability of olmesartan and amlodipine from Olbet-AM.
Olmesartan medoxomil
Absorption and distribution:
Olmesartan medoxomil is a prodrug. It is rapidly converted to the pharmacologically active metabolite, olmesartan, by esterases in the gut mucosa and in portal blood during absorption from the gastrointestinal tract. No intact olmesartan medoxomil or intact side chain medoxomil moiety have been detected in plasma or excreta. The mean absolute bioavailability of olmesartan from a tablet formulation was 25.6%.
The mean peak plasma concentration (Cmax) of olmesartan is reached within about 2 hours after oral dosing with olmesartan medoxomil, and olmesartan plasma concentrations increase approximately linearly with increasing single oral doses up to about 80 mg.
Food had minimal effect on the bioavailability of olmesartan and therefore olmesartan medoxomil may be administered with or without food.
No clinically relevant gender-related differences in the pharmacokinetics of olmesartan have been observed.
Olmesartan is highly bound to plasma protein (99.7%), but the potential for clinically significant protein binding displacement interactions between olmesartan and other highly bound coadministered active substances is low (as confirmed by the lack of a clinically significant interaction between olmesartan medoxomil and warfarin). The binding of olmesartan to blood cells is negligible. The mean volume of distribution after intravenous dosing is low (16 – 29 L).
Biotransformation and elimination:
Total plasma clearance of olmesartan was typically 1.3 L/h (CV, 19%) and was relatively slow compared to hepatic blood flow (ca 90 L/h). Following a single oral dose of 14C-labelled olmesartan medoxomil, 10% – 16% of the administered radioactivity was excreted in the urine (the vast majority within 24 hours of dose administration) and the remainder of the recovered radioactivity was excreted in the faeces. Based on the systemic availability of 25.6%, it can be calculated that absorbed olmesartan is cleared by both renal excretion (ca 40%) and hepato-biliary excretion (ca 60%). All recovered radioactivity was identified as olmesartan. No other significant metabolite was detected. Enterohepatic recycling of olmesartan is minimal. Since a large proportion of olmesartan is excreted via the biliary route, use in patients with biliary obstruction is contraindicated.
The terminal elimination half-life of olmesartan is between 10 and 15 hours after multiple oral dosing. Steady state is reached after the first few doses and no further accumulation is evident after 14 days of repeated dosing. Renal clearance is approximately 0.5 – 0.7 L/h and is independent of dose.
Drug interactions
Bile acid sequestering agent colesevelam:
Concomitant administration of 40 mg olmesartan medoxomil and 3750 mg colesevelam hydrochloride in healthy subjects resulted in 28% reduction in Cmax and 39% reduction in AUC of olmesartan. Lesser effects, 4% and 15% reduction in Cmax and AUC respectively, were observed when olmesartan medoxomil was administered 4 hours prior to colesevelam hydrochloride. Elimination half-life of olmesartan was reduced by 50 – 52% irrespectively of whether administered concomitantly or 4 hours prior to colesevelam hydrochloride.
Amlodipine
Absorption and distribution:
After oral administration of therapeutic doses, amlodipine is well absorbed with peak blood levels between 6-12 hours post dose. Absolute bioavailability has been estimated to be between 64 and 80%. The volume of distribution is approximately 21 l/kg. In vitro studies have shown that approximately 97.5% of circulating amlodipine is bound to plasma proteins.
The absorption of amlodipine is unaffected by the concomitant intake of food.
Biotransformation and elimination:
The terminal plasma elimination half-life is about 35-50 hours and is consistent with once daily dosing. Amlodipine is extensively metabolised by the liver to inactive metabolites with 10% of the parent compound and 60% of metabolites excreted in the urine.
Olmesartan medoxomil and amlodipine
Special populations
Paediatric population (age below 18 years):
No pharmacokinetic data in paediatric patients are available.
Elderly (age 65 years or over):
In hypertensive patients, the olmesartan AUC at steady state is increased by ca 35% in elderly people (65 – 75 years old) and by ca 44% in very elderly people (≥ 75 years old) compared with the younger age group (see section 4.2). This may be at least in part related to a mean decrease in renal function in this group of patients. The recommended dosage regimen for elderly people is, however, the same, although caution should be exercised when increasing the dosage.
The time to reach peak plasma concentrations of amlodipine is similar in elderly and younger subjects. Amlodipine clearance tends to be decreased with resulting increases in AUC and elimination half-life in elderly people. Increases in AUC and elimination half-life in patients with congestive heart failure were as expected for the patient age group in this study.
Renal impairment:
In renally impaired patients, the olmesartan AUC at steady state increased by 62%, 82% and 179% in patients with mild, moderate and severe renal impairment, respectively, compared to healthy controls.
Amlodipine is extensively metabolised to inactive metabolites. Ten percent of the substance is excreted unchanged in the urine. Changes in amlodipine plasma concentration are not correlated with the degree of renal impairment. In these patients, amlodipine may be administered at the normal dosage. Amlodipine is not dialysable.
Hepatic impairment:
After single oral administration, olmesartan AUC values are 6% and 65% higher in mildly and moderately hepatically impaired patients, respectively, than in their corresponding matched healthy controls. The unbound fraction of olmesartan at 2 hours post-dose in healthy subjects, in patients with mild hepatic impairment and in patients with moderate hepatic impairment is 0.26%, 0.34% and 0.41%, respectively. Following repeated dosing in patients with moderate hepatic impairment, olmesartan mean AUC is again about 65% higher than in matched healthy controls. Olmesartan mean Cmax values are similar in hepatically impaired and healthy subjects. Olmesartan medoxomil has not been evaluated in patients with severe hepatic impairment.
Very limited clinical data are available regarding amlodipine administration in patients with hepatic impairment. The clearance of amlodipine is decreased and the half-life is prolonged in patients with impaired hepatic function, resulting in an increase in AUC of about 40% – 60%.
6.0 Nonclinical properties
6.1 Animal Toxicology or Pharmacology
Based on the non-clinical toxicity profile of each substance, no exacerbation of toxicities for the combination is expected, because each substance has different targets, i.e. the kidneys for olmesartan medoxomil and the heart for amlodipine. In a 3-month, repeat-dose toxicity study of orally administered olmesartan medoxomil/amlodipine combination in rats, and the following changes were observed:
- Decreases in red blood cell count-related parameters and kidney alterations, which may be attributed to the olmesartan medoxomil component.
- Intestinal changes including luminal dilatation and diffuse mucosal thickening in the ileum and colon, which may be related to the amlodipine component.
- Adrenal alterations, such as hypertrophy of the glomerular cortical cells and vacuolation of the fascicular cortical cells, which could be induced by amlodipine.
- Hypertrophy of the mammary gland ducts, possibly induced by the amlodipine component.
These findings suggest that both components of the combination may contribute to specific organ changes, with olmesartan medoxomil primarily affecting blood cells and kidneys, and amlodipine influencing the intestines, adrenals, and mammary glands.
7.0 Description
Amlodipine and Olmesartan Medoxomil Tablets provided, as a tablet for oral administration, is a combination of the calcium channel blocker (CCB) amlodipine besylate and the angiotensin II receptor blocker (ARB) olmesartan medoxomil.
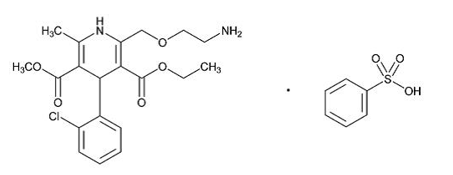
The amlodipine besylate is chemically described as 3-ethyl-5-methyl (±)-2-[(2-aminoethoxy)methyl]-4-(2-chlorophenyl)-1,4-dihydro-6-methyl-3,5-pyridinedicarboxylate, monobenzenesulphonate.
Its empirical formula is C20H25CIN2O5•C6H6O3S.
The molecular weight of amlodipine besylate is 567.1.
The structural formula for amlodipine besylate is:
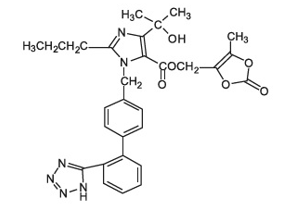
Olmesartan medoxomil, a prodrug, is hydrolyzed to olmesartan during absorption from the gastrointestinal tract.
The olmesartan medoxomil is chemically described as 2,3-dihydroxy-2-butenyl 4-(1-hydroxy-1-methylethyl)-2-propyl-1-[p-(o-1H-tetrazol-5-ylphenyl)benzyl]imidazole-5-carboxylate, cyclic 2,3-carbonate.
Its empirical formula is C29H30N6O6.
The molecular weight of olmesartan medoxomil is 558.59.
The structural formula for olmesartan medoxomil is:
8.0 Pharmaceutical particulars
8.1 Incompatibilities
Not applicable.
8.2 Shelf-life
Refer on pack
8.3 Packaging information
A Blister strip of 10 tablets each.
8.4 Storage and handing instructions
- Store below 30°C. Protected from light & moisture.
- Keep out of reach of children.
9.0 Patient counselling information
Pregnancy: Advise female patients of childbearing age about the consequences of exposure to Amlodipine and Olmesartan Medoxomil Tablets during pregnancy. Discuss treatment options with women planning to become pregnant. Tell patients to report pregnancies to their physicians as soon as possible.
Lactation: Advise nursing women not to breastfeed during treatment with Amlodipine and Olmesartan Medoxomil Tablets.
Potassium Supplements: Advise patients not to use potassium supplements or salt substitutes containing potassium without consulting their healthcare provider.
12.0 Date of revision
29/11/2024
About leaflet
Read all of this leaflet carefully before you start taking this medicine because it contains important information for you.
- Keep this leaflet. You may need to read it again.
- If you have any further questions, ask your doctor or pharmacist.
- This medicine has been prescribed for you only. Do not pass it on to others. It may harm them, even if their signs of illness are the same as yours.
- If you get any side effects, talk to your doctor or pharmacist. This includes any possible side effects not listed in this leaflet (see section 4).
What is in this leaflet:
- What Olbet-AM is and what it is used for
- What you need to know before you take Olbet-AM
- How to take Olbet-AM
- Possible side effects
- How to store Olbet-AM
- Contents of the pack and other information
1. What Olbet-AM is and what it is used for
Olbet-AM contains two substances called olmesartan medoxomil and amlodipine (as amlodipine besilate). Both of these substances help to control high blood pressure.
- Olmesartan medoxomil belongs to a group of medicines called “angiotensin-II receptor antagonists” which lower blood pressure by relaxing the blood vessels.
- Amlodipine belongs to a group of substances called “calcium channel blockers”. Amlodipine stops calcium from moving into the blood vessel wall, which stops the blood vessels from tightening thereby also reducing blood pressure.
The actions of both these substances contribute to stopping the tightening of blood vessels, so that blood vessels relax and blood pressure decreases.
Olbet AM is used for the treatment of high blood pressure in patients whose blood pressure is not controlled enough with either olmesartan medoxomil or amlodipine alone.
2. What you need to know before you take Olbet-AM
Do not take Olbet-AM
- if you are allergic to olmesartan medoxomil or to amlodipine or a special group of calcium channel blockers, the dihydropyridines, or to any of the other ingredients of this medicine (listed in section 6). If you think you may be allergic, talk to your doctor before taking Olbet AM.
- if you are more than 3 months pregnant (It is also better to avoid Olbet AM in early pregnancy - see section “Pregnancy and breastfeeding”.).
- if you have diabetes or impaired kidney function and you are treated with a blood pressure lowering medicine containing aliskiren.
- if you have severe liver problems, if bile secretion is impaired or drainage of bile from the gallbladder is blocked (e.g. by gallstones), or if you are experiencing any jaundice (yellowing of the skin and eyes).
- if you have very low blood pressure.
- if you are suffering from insufficient blood supply to your tissues with symptoms like e.g. low blood pressure, low pulse, fast heartbeat (shock, including cardiogenic shock). Cardiogenic shock means shock due to severe heart troubles.
- if the blood flow from your heart is obstructed (e.g. because of the narrowing of the aorta (aortic stenosis)).
- if you suffer from low heart output (resulting in shortness of breath or peripheral swellings) after a heart attack (acute myocardial infarction).
Warnings and precautions
Talk to your doctor or pharmacist before using Olbet-AM.
Tell your doctor if you are taking any of the following medicines used to treat high blood pressure:
- an ACE-inhibitor (for example enalapril, lisinopril, ramipril), in particular if you have diabetes-related kidney problems, ▪ aliskiren.
Your doctor may check your kidney function, blood pressure, and the amount of electrolytes (e.g. potassium) in your blood at regular intervals.
See also information under the heading “Do not take Olbet-AM”.
Tell your doctor if you have any of the following health problems:
- Kidney problems or a kidney transplant.
- Liver disease.
- Heart failure or problems with your heart valves or heart muscle.
- Severe vomiting, diarrhoea, treatment with high doses of “water tablets” (diuretics) or if you are on a low salt diet.
- Increased levels of potassium in your blood.
- Problems with your adrenal glands (hormone-producing glands on top of the kidneys).
Contact your doctor if you experience diarrhoea that is severe, persistent and causes substantial weight loss. Your doctor may evaluate your symptoms and decide on how to continue your blood pressure medication.
As with any medicine which reduces blood pressure, an excessive drop in blood pressure in patients with blood flow disturbances of the heart or brain could lead to a heart attack or stroke. Your doctor will therefore check your blood pressure carefully.
You must tell your doctor if you think that you are (or might become) pregnant. Olbet-AM is not recommended in early pregnancy, and must not be taken if you are more than 3 months pregnant, as it may cause serious harm to your baby if used at that stage (see section “Pregnancy and breast-feeding”).
Children and adolescents (under 18)
Olbet-AM is not recommended for children and adolescents under the age of 18.
Other medicines and Olbet-AM
Tell your doctor or pharmacist if you are taking, have recently taken or might take any of the following medicines:
- Other blood pressure lowering medicines, as the effect of Olbet-AM can be increased.
Your doctor may need to change your dose and/or to take other precautions: If you are taking an ACE-inhibitor or aliskiren (see also information under the headings
“Do not take Olbet-AM ” and “Warnings and precautions”).
- Potassium supplements, salt substitutes containing potassium, “water tablets” (diuretics) or heparin (for thinning the blood and prevention of blood clots.). Using these medicines at the same time as Olbet-AM may raise the levels of potassium in your blood.
- Lithium (a medicine used to treat mood swings and some types of depression) used at the same time as Olbet-AM may increase the toxicity of lithium. If you have to take lithium, your doctor will measure your lithium blood levels.
- Non-Steroidal Anti-Inflammatory Drugs (NSAIDs, medicines used to relieve pain, swelling and other symptoms of inflammation, including arthritis) used at the same time as Olbet-AM may increase the risk of kidney failure. The effect of Olbet-AM can be decreased by NSAIDs.
- Colesevelam hydrochloride, a drug that lowers the level of cholesterol in your blood, as the effect of Olbet-AM may be decreased. Your doctor may advise you to take Olbet-AM at least 4 hours before colesevelam hydrochloride.
- Certain antacids (indigestion or heartburn remedies), as the effect of Olbet-AM can be slightly decreased.
- Medicines used for HIV/AIDS (e.g. ritonavir, indinavir, nelfinavir) or for the treatment of fungal infections (e.g. ketoconazole, itraconazole).
- Diltiazem, verapamil, (agents used for heart rhythm problems and high blood pressure).
- Rifampicin, erythromycin, clarithromycin (antibiotics), agents used for tuberculosis or other infections.
- St. John’s wort (Hypericum perforatum), a herbal remedy.
- Dantrolene (infusion for severe body temperature abnormalities).
- Simvastatine, an agent used to lower levels of cholesterol and fats (triglycerides) in the blood.
- Tacrolimus, sirolimus, temsirolimus, everolimus and cyclosporine, used to control your body’s immune response, enabling your body to accept the transplanted organ.
Tell your doctor or pharmacist if you are taking, have recently taken or might take any other medicines.
Olbet-AM with food and drink
Olbet-AM can be taken with or without food. Swallow the tablet with some fluid (such as one glass of water). If possible, take your daily dose at the same time each day, for example at breakfast time. Grapefruit juice and grapefruit should not be consumed by people who are taking Olbet-AM. This is because grapefruit and grapefruit juice can lead to an increase in the blood levels of the active ingredient amlodipine, which can cause an unpredictable increase in the blood pressure lowering effect of Olbet-AM.
Elderly
If you are over 65 years of age, your doctor will regularly check your blood pressure at any dose increase, to make sure that your blood pressure does not become too low.
Black patients
As with other similar drugs the blood pressure lowering effect of Olbet-AM can be somewhat less in black patients.
Pregnancy and breast-feeding
Pregnancy
You must tell your doctor if you think that you are (or might become) pregnant. Your doctor will normally advise you to stop taking Olbet-AM before you become pregnant or as soon as you know you are pregnant and will advise you to take another medicine instead of Olbet-AM. Olbet-AM is not recommended in early pregnancy, and must not be taken when more than 3 months pregnant, as it may cause serious harm to your baby if used after the third month of pregnancy.
If you become pregnant during therapy with Olbet-AM, please inform and see your physician without delay.
Breast-feeding
Tell your doctor if you are breast-feeding or about to start breast-feeding. Amlodipine has been shown to pass into breast milk in small amounts. Olbet-AM is not recommended for mothers who are breast-feeding, and your doctor may choose another treatment for you if you wish to breast-feed, especially if your baby is newborn, or was born prematurely.
If you are pregnant or breast-feeding, think you may be pregnant or are planning to have a baby, ask your doctor or pharmacist for advice before taking this medicine.
Driving and using machines
You may feel sleepy, sick or dizzy or get a headache while being treated for your high blood pressure. If this happens, do not drive or use machines until the symptoms wear off. Ask your doctor for advice.
3. How to take Olbet-AM
Always take this medicine exactly as your doctor or pharmacist has told you. Check with your doctor or pharmacist if you are not sure.
- The recommended dose of Olbet-AM is one tablet per day.
- The tablets can be taken with or without food. Swallow the tablet with some fluid (such as a glass of water). The tablet should not be chewed. Do not take them with grapefruit juice.
- If possible, take your daily dose at the same time each day, for example at breakfast time.
If you take more Olbet-AM than you should
If you take more tablets than you should you may experience low blood pressure with symptoms such as dizziness, fast or slow heartbeat. If you take more tablets than you should or if a child accidentally swallows some, go to your doctor or nearest emergency department immediately and take your medicine pack or this leaflet with you.
Excess fluid may accumulate in your lungs (pulmonary oedema) causing shortness of breath that may develop up to 24-48 hours after intake.
If you forget to take Olbet-AM
If you forget to take a dose, take your normal dose on the following day as usual. Do not take a double dose to make up for a forgotten dose.
If you stop taking Olbet-AM
It is important to continue to take Olbet-AM unless your doctor tells you to stop.
If you have any further questions on the use of this medicine, ask your doctor or pharmacist.
4. Possible side effects
Like all medicines, this medicine can cause side effects, although not everybody gets them. If they do occur, they are often mild and do not require treatment to be stopped.
Although not many people may get them, the following side effects can be serious:
Allergic reactions, that may affect the whole body, with swelling of the face, mouth and/or larynx (voice box) together with itching and rash may occur during treatment with Olbet-AM. If this happens stop taking Olbet-AM and talk to your doctor immediately.
Olbet-AM can cause the blood pressure to fall too low in susceptible individuals or as the result of an allergic reaction. This could cause severe light-headedness or fainting. If this happens stop taking Olbet-AM, talk to your doctor immediately and lie down flat.
Frequency not known: If you experience yellowing of the whites of the eyes, dark urine, itching of the skin, even if you started therapy with Olbet-AM longer time ago, contact your doctor immediately who will evaluate your symptoms and decide on how to continue your blood pressure medication.
Other possible side effects with Olbet-AM:
Common (may affect less than 1 in 10 people):
Dizziness; headache; swelling of ankles, feet, legs, hands, or arms; tiredness.
Uncommon (may affect less than 1 in 100 people):
Dizziness on standing up; lack of energy; tingling or numbness of hands or feet; vertigo; awareness of heart beat; fast heart beat; low blood pressure with symptoms such as dizziness, light-headedness; difficult breathing; cough; nausea; vomiting; indigestion; diarrhoea; constipation; dry mouth, upper abdominal pain; skin rash; cramps; pain in arms and legs; back pain; feeling more of an urge to pass urine; sexual inactivity; inability to get or maintain an erection; weakness.
Some changes in blood test results have also been seen and include the following: increased as well as decreased blood potassium levels, increased blood creatinine levels, increased uric acid levels, increases in a test of liver function (gamma glutamyl transferase levels).
Rare (may affect less than 1 in 1,000 people):
Drug hypersensitivity; fainting; redness and warm feeling of the face; red itchy bumps (hives); swelling of face.
Side effects reported with use of olmesartan medoxomil or amlodipine alone, but not with Olbet-AM or in a higher frequency:
Olmesartan medoxomil
Common (may affect less than 1 in 10 people):
Bronchitis; sore throat; runny or stuffy nose; cough; abdominal pain; stomach flu; diarrhoea; indigestion; nausea; pain in the joints or bones; back pain; blood in the urine; infection of the urinary tract; chest pain; flu-like symptoms; pain. Changes in blood test results as increased fat levels (hypertriglyceridaemia), blood urea or uric acid increased and increase in tests of liver and muscle function.
Uncommon (may affect less than 1 in 100 people):
Reduced number of a type of blood cells, known as platelets, which can result in easily bruising or prolonged bleeding time; quick allergic reactions that may affect the whole body and may cause breathing problems as well as a rapid fall of blood pressure that may even lead to fainting (anaphylactic reactions); angina (pain or uncomfortable feeling in the chest, known as angina pectoris); itching; eruption of the skin; allergic skin rash; rash with hives; swelling of the face; muscular pain; feeling unwell.
Rare (may affect less than 1 in 1,000 people):
Swelling of the face, mouth and/or larynx (voice box); acute kidney failure and kidney insufficiency; lethargy.
Amlodipine
Very common (may affect more than 1 in 10 people):
Oedema (fluid retention)
Common (may affect less than 1 in 10 people):
Abdominal pain; nausea; ankle swelling; feeling sleepy; redness and warm feeling of the face, visual disturbance (including double vision and blurred vision), awareness of heartbeat, diarrhoea, constipation, indigestion, cramps, weakness, difficult breathing.
Uncommon (may affect less than 1 in 100 people):
Trouble sleeping; sleep disturbances; mood changes including feeling anxious; depression; irritability; shiver; taste changes; fainting; ringing in the ears (tinnitus); worsening of angina pectoris (pain or uncomfortable feeling in the chest); irregular heartbeat; runny or stuffy nose; loss of hair; purplish spots or patches on the skin due to small haemorrhages (purpura); discoloration of the skin; excessive sweating; eruption of the skin; itching; red itchy bumps (hives); pain of joints or muscles; problems to pass urine; urge to pass urine at night; increased need to urinate (pass urine); breast enlargement in men; chest pain; pain, feeling unwell; increase or decrease in weight.
Rare (may affect less than 1 in 1,000 people):
Confusion
Very rare (may affect less than 1 in 10,000 people):
Reduction in the number of white cells in the blood, which could increase the risk of infections; a reduction in the number of a type of blood cells known as platelets, which can result in easily bruising or prolonged bleeding time; increase in blood glucose; increased tightness of muscles or increased resistance to passive movement (hypertonia); tingling or numbness of hands or feet; heart attack; inflammation of blood vessels; inflammation of the liver or the pancreas; inflammation of stomach lining; thickening of gums; elevated liver enzymes; yellowing of the skin and eyes; increased sensitivity of the skin to light; allergic reactions: itching, rash, swelling of the face, mouth and/or larynx (voice box) together with itching and rash, severe skin reactions including intense skin rash, hives, reddening of the skin over your whole body, severe itching, blistering, peeling and swelling of the skin, inflammation of mucous membranes (Stevens Johnson Syndrome, toxic epidermal necrolysis), sometimes life-threatening.
Not known (frequency cannot be estimated from the available data): Trembling, rigid posture, mask-like face, slow movements and a shuffling, unbalanced walk.
Reporting of side effects
If you get any side effects, talk to your doctor. This includes any possible side effects not listed in this leaflet. You can also report side effects directly: Website: www.zuventus.com and click the tab “Safety Reporting” located on the top end of the home page.
By reporting side effects, you can help provide more information on the safety of this medicine.
5. How to store Olbet-AM
Keep this medicine out of the sight and reach of children.
Do not use this medicine after the expiry date which is stated on the carton after EXP. The expiry date refers to the last day of that month.
- Store below 30°C. Protected from light & moisture.
- Keep out of reach of children.
6. Contents of the pack and other information
What Olbet AM contains
The active substances are olmesartan medoxomil and amlodipine (as besilate).
Olbet AM 20: Each tablet contains 20 mg of olmesartan medoxomil and 5 mg amlodipine (as besilate).
Olbet AM 40: Each tablet contains 40 mg of olmesartan medoxomil and 5 mg amlodipine (as besilate).
Marketing Authorisation Holder and Manufacturer
Zuventus Healthcare Ltd.
Zuventus House, Plot No. Y2,
near Nahur Railway Station, off Raycon IT Park Road,
Nahur West, Industrial Area, Mumbai, Maharashtra 400078
This leaflet was last revised in November 2024.