Supexa- OD 60 Tablets

1.0 Generic name
Edoxaban Tablets
2.0 Qualitative and quantitative composition
SUPEXA OD 15
Each film-coated tablet contains
Edoxaban Tosylate Monohydrate
equivalent to Edoxaban ……….15 mg
Excipient…………………….q.s
Colours: Yellow Oxide of Iron and Titanium Dioxide IP
SUPEXA OD 30
Each film-coated tablet contains
Edoxaban Tosylate Monohydrate
equivalent to Edoxaban ……….30 mg
Excipient…………………….q.s
Colours: Yellow Oxide of Iron and Titanium Dioxide IP
SUPEXA OD 60
Each film-coated tablet contains
Edoxaban Tosylate Monohydrate
equivalent to Edoxaban ……….60 mg
Excipient…………………….q.s
Colours: Yellow Oxide of Iron and Titanium Dioxide IP
3.0 Dosage form and strength
Film coated tablet, 15 mg / 30 mg / 60 mg
4.0 Clinical particulars
4.1Therapeutic indications
- For prevention of stroke and systemic embolism in adult patients with nonvalvular atrial fibrillation (NVAF) with one or more risk factors, such as congestive heart failure, hypertension, age ≥ 75 years, diabetes mellitus, prior stroke or transient ischaemic attack (TIA).
- For the treatment of deep vein thrombosis (DVT) and pulmonary embolism (PE), and for the prevention of recurrent DVT and PE in adults.
4.2 Posology and method of administration
Posology
Prevention of stroke and systemic embolism
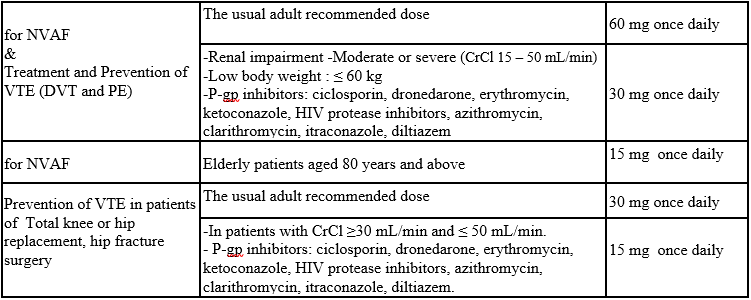
- The recommended dose is 60 mg edoxaban once daily. Therapy with edoxaban in NVAF patients should be continued long term.
- The recommended dose is 30 mg edoxaban once daily in patients with one or more of the following clinical factors:
- Moderate or severe renal impairment (creatinine clearance (CrCl) 15 - 50 mL/min)
- Low body weight ≤ 60 kg
- Concomitant use of the following P-glycoprotein (P-gp) inhibitors: ciclosporin, dronedarone, erythromycin, ketoconazole, HIV protease inhibitors, azithromycin, clarithromycin, itraconazole, diltiazem.
- For elderly patients aged 80 years and above: dose reduced to 15 mg once daily.
Treatment of DVT, PE and prevention of recurrent DVT and PE (venous thromboembolism (VTE))
- The recommended dose is 60 mg edoxaban once daily following initial use of parenteral anticoagulant for at least 5 days. Edoxaban and initial parenteral anticoagulant should not be administered simultaneously. The duration of therapy for treatment of DVT and PE (VTE), and prevention of recurrent VTE should be individualized after careful assessment of the treatment benefit against the risk for bleeding. Short duration of therapy (at least 3 months) should be based on transient risk factors (e.g. recent surgery, trauma, immobilization) and longer durations should be based on permanent risk factors or idiopathic DVT or PE.
- The recommended dose is 30 mg edoxaban once daily in patients with one or more of the following clinical factors:
- Moderate to severe renal impairment (CrCl -15 - 50 mL/min)
- Low body weight ≤ 60 kg
- Concomitant use of P-glycoprotein (P-gp) inhibitors: ciclosporin, dronedarone, erythromycin, ketoconazole, HIV protease inhibitors, azithromycin, clarithromycin, itraconazole, diltiazem.
- Prevention of venous thromboembolism (VTE) in patients undergoing orthopedic surgery for the lower limbs - Total knee or hip replacement, hip fracture surgery:
- The usual adult dosage is 30 mg of edoxaban administered orally once daily.
- Consider reducing the dose to 15 mg once daily if
- Renal impairment (CrCl 30 mL/min and ≤ 50 mL/min).
- Concomitant use of P-glycoprotein (P-gp) inhibitors: ciclosporin, dronedarone, erythromycin, ketoconazole, HIV protease inhibitors, azithromycin, clarithromycin, itraconazole, diltiazem.
- Edoxaban should be administered 12 hours after surgery and after confirming that there is no bleeding from the surgical wound, etc.
- Edoxaban should be at least 2 hours after the epidural catheter is removed or lumbar puncture is performed.
Table 1: Summary of Edoxaban Posology in NVAF and VTE (DVT and PE)
Missed dose
If a dose of edoxaban is missed, the dose should be taken immediately and then be continued the following day with the once-daily intake as recommended. The patient should not take double the prescribed dose on the same day to make up for a missed dose. Switching to and from edoxaban Continued anticoagulant therapy is important in patients with NVAF and VTE. There may be situations that warrant a change in anticoagulation therapy (Table 2).
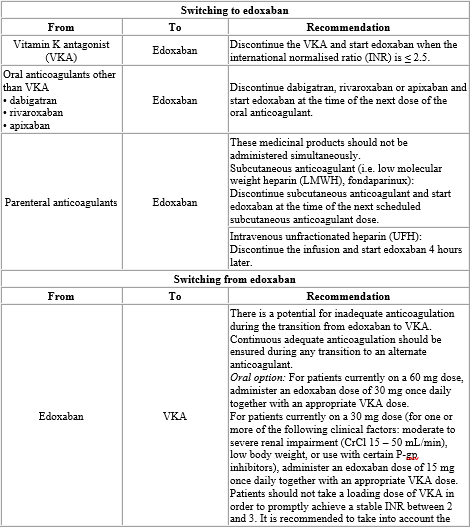
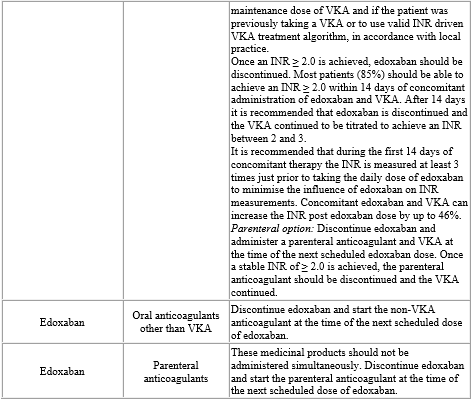
Table 2: Switching of anticoagulant treatment in NVAF and VTE (DVT and PE)
Special populations
Elderly population
No dose reduction is required.
Renal impairment
Renal function should be assessed in all patients by calculating the CrCl prior to initiation of treatment with edoxaban to exclude patients with end stage renal disease (i.e. CrCl < 15 mL/min), to use the correct edoxaban dose in patients with CrCl 15 – 50 mL/min (30 mg once daily), in patients with CrCl > 50 mL/min (60 mg once daily) and when deciding on the use of edoxaban in patients with increased CrCl.
Renal function should also be assessed when a change in renal function is suspected during treatment (e.g. hypovolaemia, dehydration, and in case of concomitant use of certain medicinal products).
The method used to estimate renal function (CrCl in mL/min) during the clinical development of edoxaban was the Cockcroft-Gault method. The formula is as follows:
For creatinine in µ mol/L:
1.23× (140-age [years])× weight [kg] (× 0.85 if Female)
Serum creatinine [µmol/L]
For creatinine in mg/dL:
(140-age [years]) × weight [kg] (× 0.85 if Female)
72×Serum creatinine [mg/dL]
This method is recommended when assessing patients' CrCl prior to and during edoxaban treatment.
In patients with mild renal impairment (CrCl > 50 – 80 mL/min), the recommended dose is 60 mg edoxaban once daily.
In patients with moderate or severe renal impairment (CrCl 15 – 50 mL/min), the recommended dose is 30 mg edoxaban once daily.
In patients with end stage renal disease (ESRD) (CrCl < 15 mL/min) or on dialysis, the use of edoxaban is not recommended.
Hepatic impairment
Edoxaban is contraindicated in patients with hepatic disease associated with coagulopathy and clinically relevant bleeding risk.
In patients with severe hepatic impairment edoxaban is not recommended.
In patients with mild to moderate hepatic impairment the recommended dose is 60 mg edoxaban once daily. Edoxaban should be used with caution in patients with mild to moderate hepatic impairment.
Patients with elevated liver enzymes (alanine aminotransferase (ALT) or aspartate transaminase (AST) > 2 x upper limit of normal (ULN)) or total bilirubin ≥ 1.5 x ULN, were excluded in clinical studies. Therefore, edoxaban should be used with caution in this population. Prior to initiating edoxaban, liver function testing should be performed.
Body weight
For patients with body weight ≤ 60 kg, the recommended dose is 30 mg edoxaban once daily).
Gender
No dose reduction is required.
Concomitant use of edoxaban with P-glycoprotein (P-gp) inhibitors
In patients concomitantly taking edoxaban and the following P-gp inhibitors: ciclosporin, dronedarone, erythromycin, ketoconazole, HIV protease inhibitors, azithromycin, clarithromycin, itraconazole, diltiazem, the recommended dose is 30 mg edoxaban once daily.
No dose reduction is required for concomitant use of amiodarone, quinidine or verapamil. The use of edoxaban with other P-gp inhibitors including HIV protease inhibitors has not been studied.
Patients undergoing cardioversion
Edoxaban can be initiated or continued in patients who may require cardioversion. For transoesophageal echocardiogram (TEE) guided cardioversion in patients not previously treated with anticoagulants, edoxaban treatment should be started at least 2 hours before cardioversion to ensure adequate anticoagulation. Cardioversion should be performed no later than 12 hours after the dose of edoxaban on the day of the procedure.
For all patients undergoing cardioversion: Confirmation should be sought prior to cardioversion that the patient has taken edoxaban as prescribed. Decisions on initiation and duration of treatment should follow established guidelines for anticoagulant treatment in patients undergoing cardioversion.
Paediatric population
Edoxaban is not recommended for use in children and adolescents from birth to 18 years of age with confirmed VTE (PE and/or DVT) event as the efficacy has not been established.
Method of administration
For oral use.
Edoxaban can be taken with or without food.
For patients who are unable to swallow whole tablets, edoxaban tablets may be crushed and mixed with water or apple puree and immediately administered orally. Alternatively, edoxaban tablets may be crushed and suspended in a small amount of water and immediately delivered through a nasogastric tube or gastric feeding tube after which it should be flushed with water. Crushed edoxaban tablets are stable in water and apple puree for up to 4 hours.
4.3 Contraindications
- Hypersensitivity to the active substance or to any of the excipients listed in the formulation.
- Clinically significant active bleeding.
- Hepatic disease associated with coagulopathy and clinically relevant bleeding risk.
- Lesion or condition, if considered to be a significant risk for major bleeding. This may include current or recent gastrointestinal ulceration, presence of malignant neoplasms at high risk of bleeding, recent brain or spinal injury, recent brain, spinal or ophthalmic surgery, recent intracranial haemorrhage, known or suspected oesophageal varices, arteriovenous malformations, vascular aneurysms or major intraspinal or intracerebral vascular abnormalities.
- Uncontrolled severe hypertension.
- Concomitant treatment with any other anticoagulants e.g. UFH, LMWH (enoxaparin, dalteparin, etc.), heparin derivatives (fondaparinux, etc.), oral anticoagulants (warfarin, dabigatran etexilate, rivaroxaban, apixaban etc.) except under specific circumstances of switching oral anticoagulant therapy or when UFH is given at doses necessary to maintain an open central venous or arterial catheter.
- Pregnancy and breast-feeding.
4.4 Special warnings and precautions for use
Edoxaban 15 mg is not indicated as monotherapy, as it may result in decreased efficacy. It is only indicated in the process of switching from edoxaban 30 mg (patients with one or more clinical factors for increased exposure; see table 1) to VKA, together with an appropriate VKA dose.
Haemorrhagic risk
Edoxaban increases the risk of bleeding and can cause serious, potentially fatal bleeding. Edoxaban, like other anticoagulants, is recommended to be used with caution in patients with increased risk of bleeding. Edoxaban administration should be discontinued if severe haemorrhage occurs.
In the clinical studies mucosal bleedings (e.g. epistaxis, gastrointestinal, genitourinary) and anaemia were seen more frequently during long term edoxaban treatment compared with VKA treatment. Thus, in addition to adequate clinical surveillance, laboratory testing of haemoglobin/haematocrit could be of value to detect occult bleeding, as judged to be appropriate.
Several sub-groups of patients, as detailed below, are at increased risk of bleeding. These patients are to be carefully monitored for signs and symptoms of bleeding complications and anaemia after initiation of treatment. Any unexplained fall in haemoglobin or blood pressure should lead to a search for a bleeding site.
The anticoagulant effect of edoxaban cannot be reliably monitored with standard laboratory testing. A specific anticoagulant reversal agent for edoxaban is not available. Haemodialysis does not significantly contribute to edoxaban clearance.
Elderly
The co-administration of edoxaban with acetylsalicylic acid (ASA) in elderly patients should be used cautiously because of a potentially higher bleeding risk.
Renal impairment
The plasma area under the curve (AUC) for subjects with mild (CrCl > 50 - 80 mL/min), moderate (CrCl 30 - 50 mL/min) and severe (CrCl < 30 mL/min but not undergoing dialysis) renal impairment was increased by 32%, 74%, and 72%, respectively, relative to subjects with normal renal function. In patients with end stage renal disease or on dialysis, edoxaban is not recommended.
Renal function in NVAF A trend towards decreasing efficacy with increasing CrCl was observed for edoxaban compared to well-managed warfarin.
Edoxaban should be used in patients with NVAF and high CrCl only after a careful evaluation of the individual thromboembolic and bleeding risk.
Assessment of renal function: CrCl should be monitored at the beginning of the treatment in all patients and afterwards when clinically indicated.
Hepatic impairment
Edoxaban is not recommended in patients with severe hepatic impairment. Edoxaban should be used with caution in patients with mild or moderate hepatic impairment.
Patients with elevated liver enzymes (ALT/AST > 2 x ULN) or total bilirubin ≥ 1.5 x ULN were excluded in clinical studies. Therefore, edoxaban should be used with caution in this population. Prior to initiating edoxaban, liver function testing should be performed. Periodic hepatic monitoring is recommended for patients on edoxaban treatment beyond 1 year.
Discontinuation for surgery and other interventions
If anticoagulation must be discontinued to reduce the risk of bleeding with surgical or other procedures, edoxaban should be stopped as soon as possible and preferably at least 24 hours before the procedure.
In deciding whether a procedure should be delayed until 24 hours after the last dose of edoxaban, the increased risk of bleeding should be weighed against the urgency of the intervention. Edoxaban should be restarted after the surgical or other procedures as soon as adequate haemostasis has been established, noting that the time to onset of the edoxaban anticoagulant therapeutic effect is 1 – 2 hours. If oral medicinal products cannot be taken during or after surgical intervention, consider administering a parenteral anticoagulant and then switch to oral once daily edoxaban.
Interaction with other medicinal products affecting haemostasis
Concomitant use of medicinal products affecting haemostasis may increase the risk of bleeding. These include ASA, P2Y12 platelet inhibitors, other antithrombotic agents, fibrinolytic therapy, selective serotonin reuptake inhibitors (SSRIs) or serotonin norepinephrine reuptake inhibitors (SNRIs), and chronic nonsteroidal anti-inflammatory drugs (NSAIDs).
Prosthetic heart valves and moderate to severe mitral stenosis
Edoxaban has not been studied in patients with mechanical heart valves, in patients during the first 3 months after implantation of a bioprosthetic heart valve, with or without atrial fibrillation, or in patients with moderate to severe mitral stenosis. Therefore, use of edoxaban is not recommended in these patients.
Haemodynamically unstable PE patients or patients who require thrombolysis or pulmonary embolectomy
Edoxaban is not recommended as an alternative to UFH in patients with pulmonary embolism who are haemodynamically unstable or may receive thrombolysis or pulmonary embolectomy since the safety and efficacy of edoxaban have not been established in these clinical situations.
Patients with active cancer
Efficacy and safety of edoxaban in the treatment and/or prevention of VTE in patients with active cancer have not been established.
Patients with antiphospholipid syndrome
Direct acting oral anticoagulants (DOACs) including edoxaban are not recommended for patients with a history of thrombosis who are diagnosed with antiphospholipid syndrome. In particular for patients that are triple positive (for lupus anticoagulant, anticardiolipin antibodies, and anti-beta 2-glycoprotein I antibodies), treatment with DOACs could be associated with increased rates of recurrent thrombotic events compared with vitamin K antagonist therapy.
Laboratory coagulation parameters
Although treatment with edoxaban does not require routine monitoring, the effect on anticoagulation can be estimated by a calibrated quantitative anti-Factor Xa (anti-FXa) assay which may help to inform clinical decisions in particular situations as, e.g. overdose and emergency surgery.
Edoxaban prolongs standard clotting tests such as prothrombin time (PT), INR, and activated partial thromboplastin time (aPTT) as a result of Factor Xa (FXa) inhibition. Changes observed in these clotting tests at the expected therapeutic dose are, however, small, subject to a high degree of variability, and not useful in monitoring the anticoagulation effect of edoxaban.
4.5 Drug interactions
Edoxaban is predominantly absorbed in the upper gastrointestinal (GI) tract. Thus, medicinal products or disease conditions that increase gastric emptying and gut motility have the possibility of reducing edoxaban dissolution and absorption.
P-gp inhibitors
Edoxaban is a substrate for the efflux transporter P-gp. In pharmacokinetic (PK) studies, concomitant administration of edoxaban with the P-gp inhibitors ciclosporin, dronedarone, erythromycin, ketoconazole, quinidine, or verapamil resulted in increased plasma concentrations of edoxaban. Concomitant use of edoxaban with ciclosporin, dronedarone, erythromycin, ketoconazole, HIV protease inhibitors, azithromycin, clarithromycin, itraconazole, diltiazem requires dose reduction to 30 mg once daily. Concomitant use of edoxaban with quinidine, verapamil, or amiodarone does not require dose reduction based on clinical data.
The use of edoxaban with other P-gp inhibitors including human immunodeficiency virus (HIV) protease inhibitors has not been studied.
Edoxaban 30 mg instead of 60 mg once daily must be administered during concomitant use with the following P-gp inhibitors:
- Ciclosporin: Concurrent administration of a single dose of ciclosporin 500 mg with a single dose of edoxaban 60 mg increased edoxaban AUC and maximum serum concentration (Cmax) by 73% and 74%, respectively.
- Dronedarone: Dronedarone 400 mg twice daily for 7 days with a single concomitant dose of edoxaban 60 mg on day 5 increased edoxaban AUC and Cmax by 85% and 46%, respectively.
- Erythromycin: Erythromycin 500 mg four times daily for 8 days with a single concomitant dose of edoxaban 60 mg on day 7 increased the edoxaban AUC and Cmax by 85% and 68%, respectively.
- Ketoconazole: Ketoconazole 400 mg once daily for 7 days with a single concomitant dose of edoxaban 60 mg on day 4, increased edoxaban AUC and Cmax by 87% and 89%, respectively.
Edoxaban 60 mg once daily is recommended during concomitant use with the following P-gp inhibitors:
- Quinidine: Quinidine 300 mg once daily on days 1 and 4 and three times daily on days 2 and 3, with a single concomitant dose of edoxaban 60 mg on day 3, increased edoxaban AUC over 24 hours by 77% and Cmax by 85%, respectively.
- Verapamil: Verapamil 240 mg once daily for 11 days with a single concomitant dose of edoxaban 60 mg on day 10 increased the edoxaban AUC and Cmax by approximately 53%.
- Amiodarone: Co-administration of amiodarone 400 mg once daily with edoxaban 60 mg once daily increased AUC by 40% and Cmax by 66%. This was not considered clinically significant. In ENGAGE AF-TIMI 48 study in NVAF, efficacy and safety results were similar for subjects with and without concomitant amiodarone use.
P-gp inducers
Co-administration of edoxaban with the P-gp inducer rifampicin led to a decrease in mean edoxaban AUC and a shortened half-life, with possible decreases in its pharmacodynamic effects. The concomitant use of edoxaban with other P-gp inducers (e.g. phenytoin, carbamazepine, phenobarbital or St. John's Wort) may lead to reduced edoxaban plasma concentrations. Edoxaban should be used with caution when co-administered with P-gp inducers.
P-gp substrates
Digoxin
Edoxaban 60 mg once daily on days 1 to 14 with co administration of multiple daily doses of digoxin 0.25 mg twice daily (days 8 and 9) and 0.25 mg once daily (days 10 to 14) increased the Cmax of edoxaban by 17%, with no significant effect on AUC or renal clearance at steady state. When the effects of edoxaban on digoxin PK were also examined, the Cmax of digoxin increased by approximately 28% and AUC by 7%. This was not considered clinically relevant. No dose modification is necessary when edoxaban is administered with digoxin.
Anticoagulants, antiplatelet, NSAIDs and SSRIs/SNRIs
Anticoagulants
Co-administration of edoxaban with other anticoagulants is contraindicated due to increased risk of bleeding.
ASA
Co-administration of ASA (100 mg or 325 mg) and edoxaban increased bleeding time relative to either medicinal product alone. Co-administration of high dose ASA (325 mg) increased the steady state Cmax and AUC of edoxaban by 35% and 32%, respectively. The concomitant chronic use of high dose ASA (325 mg) with edoxaban is not recommended. Concomitant administration of higher doses than 100 mg ASA should only be performed under medical supervision.
In clinical studies concomitant use of ASA (low dose ≤ 100 mg/day), other antiplatelet agents, and thienopyridines was permitted and resulted in approximately a 2-fold increase in major bleeding in comparison with no concomitant use, although to a similar extent in the edoxaban and warfarin groups. Co-administration of low dose ASA (≤ 100 mg) did not affect the peak or total exposure of edoxaban either after single dose or at steady-state. Edoxaban can be co-administered with low dose ASA (≤ 100 mg/day).
Platelet inhibitors
In ENGAGE AF-TIMI 48 concomitant use of thienopyridines (e.g. clopidogrel) monotherapy was permitted and resulted in increased clinically relevant bleeding although with a lower risk of bleeding on edoxaban compared to warfarin.
There is very limited experience on the use of edoxaban with dual antiplatelet therapy or fibrinolytic agents.
NSAIDs
Co-administration of naproxen and edoxaban increased bleeding time relative to either medicinal product alone. Naproxen had no effect on the Cmax and AUC of edoxaban. In clinical studies, co-administration of NSAIDs resulted in increased clinically relevant bleeding. Chronic use of NSAIDs with edoxaban is not recommended.
SSRIs/SNRIs
As with other anticoagulants the possibility may exist that patients are at increased risk of bleeding in case of concomitant use with SSRIs or SNRIs due to their reported effect on platelets.
Effect of edoxaban on other medicinal products
Edoxaban increased the Cmax of concomitantly administered digoxin by 28%; however, the AUC was not affected. Edoxaban had no effect on the Cmax and AUC of quinidine. Edoxaban decreased the Cmax and AUC of concomitantly administered verapamil by 14% and 16%, respectively.
4.6 Use in special populations (such as pregnant woman, lactating women, paediatric patients, geriatric patients etc.)
Women of childbearing potential
Women of childbearing potential should avoid becoming pregnant during treatment with edoxaban.
Pregnancy
Safety and efficacy of edoxaban have not been established in pregnant women. Studies in animals have shown reproductive toxicity. Due to the potential reproductive toxicity, the intrinsic risk of bleeding and the evidence that edoxaban passes the placenta, Supexa OD is contraindicated during pregnancy.
Breast-feeding
Safety and efficacy of edoxaban have not been established in breast-feeding women. Data from animals indicate that edoxaban is secreted into breast milk. Therefore, Supexa OD is contraindicated during breast-feeding. A decision must be made whether to discontinue breast-feeding or to discontinue/abstain from therapy.
Fertility
No specific studies with edoxaban in human beings have been conducted to evaluate effects on fertility. In a study on male and female fertility in rats no effects were seen
4.7 Effects on ability to drive and use machines
Edoxaban has no or negligible influence on the ability to drive and use machines.
4.8 Undesirable effects
Summary of the safety profile
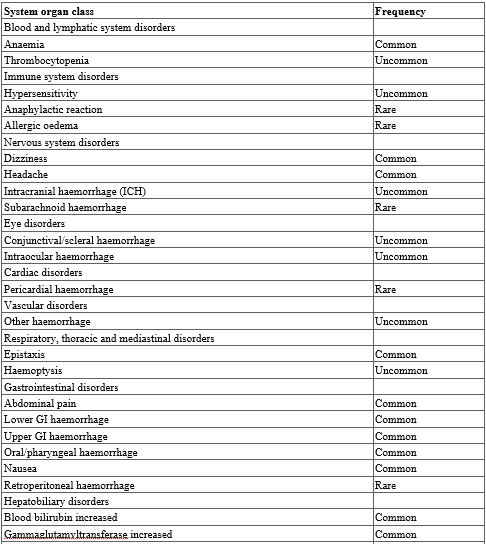
The most commonly reported adverse reactions associated with edoxaban treatment are epistaxis, haematuria and anaemia. Bleeding can occur at any site and may be severe and even fatal.
Table 3. Tabulated list of adverse reactions
Reporting of side effects
Reporting suspected adverse reactions after authorization of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via
email to: medico@zuventus.com
Website: https://www.zuventus.co.in/drug-safety-reporting
By reporting side effects, you can help provide more information on the safety of this medicine.
4.9 Overdose
Overdose
Overdose with Edoxaban may lead to haemorrhage. Experience with overdose cases is very limited. Studies have confirmed that Andexanet alfa, a modifed recombinant inactive form of human factor Xa that binds to and blocks the effects of factor Xa inhibitors can be used as an antidote1,2. Early administration of activated charcoal may be considered in case of Edoxaban overdose to reduce absorption. This recommendation is based on standard treatment of medicinal product overdose and data available with similar compounds, as the use of activated charcoal to reduce absorption of Edoxaban has not been specifically studied in the Edoxaban clinical programme.
Management of bleeding :
Should a bleeding complication arise in a patient receiving Edoxaban, the next Edoxaban administration should be delayed or treatment should be discontinued as appropriate. Edoxaban has a half-life of approximately 10 to 14 hours. Management should be individualized according to the severity and location of the haemorrhage. Appropriate symptomatic treatment could be used as needed, such as mechanical compression (e.g. for severe epistaxis), surgical haemostasis with bleeding control procedures, fluid replacement and haemodynamic support, blood products (packed red cells or fresh frozen plasma, depending on associated anaemia or coagulopathy) or platelets. For life-threatening bleeding that cannot be controlled with the measures such as transfusion or haemostasis, the administration of a 4-factor prothrombin complex concentrate (PCC) at 50 IU/kg has been shown to reverse the effects of Edoxaban 30 minutes after completing the infusion.
Recombinant factor VIIa (r-FVIIa) can also be considered. However, there is limited clinical experience with the use of this product in individuals receiving Edoxaban. Depending on local availability, a consultation with a coagulation expert should be considered in case of major bleedings. Protamine sulfate and vitamin K are not expected to affect the anticoagulant activity of Edoxaban. There is no experience with antifibrinolytic agents (Tranexamic acid, Aminocaproic acid) in individuals receiving Edoxaban. There is neither scientific rationale for benefit nor experience with the use of systemic haemostatics (Desmopressin, Aprotinin) in individuals receiving Edoxaban. Due to the high plasma protein binding Edoxaban is not expected to be dialyzable.
5.0 Pharmacological properties
5.1 Mechanism of action
Edoxaban is a highly selective, direct and reversible inhibitor of FXa, the serine protease located in the final common pathway of the coagulation cascade. Edoxaban inhibits free FXa, and prothrombinase activity. Inhibition of FXa in the coagulation cascade reduces thrombin generation, prolongs clotting time and reduces the risk of thrombus formation.
5.2 Pharmacodynamic properties
Edoxaban produces rapid onset of pharmacodynamic effects within 1 - 2 hours, which corresponds with peak Edoxaban exposure (Cmax). The pharmacodynamic effects measured by anti-FXa assay are predictable and correlate with the dose and the concentration of Edoxaban. As a result of FXa inhibition, Edoxaban also prolongs clotting time in tests such as PT and aPTT. Changes observed in these clotting tests are expected at the therapeutic dose, however, these changes are small, subject to a high degree of variability, and not useful in monitoring the anticoagulation effect of Edoxaban.
Effects of coagulation markers when switching from Rivaroxaban, Dabigatran or Apixaban to Edoxaban : In clinical pharmacology studies, healthy subjects received Rivaroxaban 20 mg once daily, Dabigatran 150 mg twice daily or Apixaban 5 mg twice daily, followed by a single dose of Edoxaban 60 mg on day 4. The effect on PT and other coagulation biomarkers (e.g. anti-FXa, aPTT) was measured. Following the switch to Edoxaban on day 4 the PT was equivalent to day 3 of Rivaroxaban and Apixaban. For dabigatran higher aPTT activity was observed after Edoxaban administration with prior Dabigatran treatment compared to that after treatment with Edoxaban alone. This is considered to be due to the carry-over effect of dabigatran treatment, however, this did not lead to a prolongation of bleeding time.
Based on these data, when switching from these anticoagulants to Edoxaban, the first dose of Edoxaban can be initiated at the time of the next scheduled dose of the previous anticoagulant
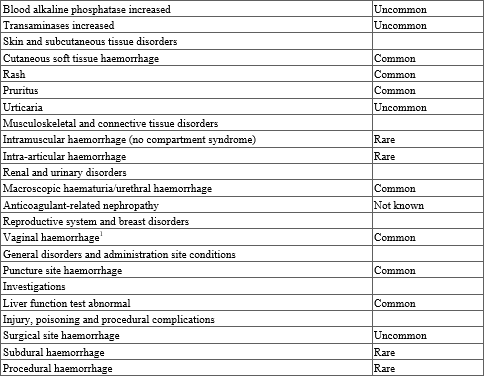
5.3 Pharmacokinetic properties
The pharmacokinetic parameters of Edoxaban in plasma after a single dose of Supexa OD 60 were as follows.
Absorption : Edoxaban is absorbed with peak plasma concentrations within 1 - 2 hours following oral administration of Edoxaban tablets. The absolute bioavailability is approximately 62%. Food increases peak exposure of Edoxaban tablets to a varying extent, but has minimal effect on total exposure.Edoxaban is poorly soluble at pH of 6.0 or higher. Co-administration of proton-pump inhibitors had no relevant impact on Edoxaban exposure.
In a study with 30 healthy subjects, both mean AUC and Cmax values for 60 mg Edoxaban administered as a crushed tablet orally mixed in apple puree or via nasogastric tube suspended in water were bioequivalent to the intact tablet. Given the predictable, dose-proportional pharmacokinetic profile of Edoxaban, the bioavailability results from this study are likely applicable to lower Edoxaban doses.
Distribution : Disposition is biphasic. The volume of distribution is 107 (19.9) L mean (SD). In vitro plasma protein binding is approximately 55%. There is no clinically relevant accumulation of Edoxaban (accumulation ratio 1.14) with once daily dosing. Steady state concentrations are achieved within 3 days.
Biotransformation : Unchanged Edoxaban is the predominant form in plasma. Edoxaban is metabolized via hydrolysis (mediated by carboxylesterase 1), conjugation or oxidation by CYP3A4/5 (< 10%). Edoxaban has three active metabolites, the predominant metabolite (M-4), formed by hydrolysis, is active and reaches less than 10% of the exposure of the parent compound in healthy subjects. Exposure to the other metabolites is less than 5%. Edoxaban is a substrate for the efflux transporter P-gp, but not a substrate for uptake transporters such as organic anion transporter polypeptide OATP1B1, organic anion transporters OAT1 or OAT3 or organic cation transporter OCT2. Its active metabolite is a substrate for OATP1B1.
Elimination : In healthy subjects, the total clearance is reported as 22 (± 3) L/hour; 50% is renally cleared (11 L/hour). Renal clearance accounts for approximately 35% of the administered dose. Metabolism and biliary / intestinal excretion account for the remaining clearance.
6.0 Nonclinical properties
6.1 Animal toxicology or pharmacology
Acute oral toxicity study in rat and mice : A daily oral administration of Edoxaban Tosylate Monohydrate was given for 14 consecutive days to twenty-five Wistar Rats and twenty-five Swiss Albino Mice (5 per group). Each group (G1, G2, G3, G4, and G5) was administered a dose of 0, 250, 500, 1000 and 2000 mg/kg bw respectively. No mortality was observed in any dose group throughout the experiment period. All animals appeared normal throughout the study period. No external or internal gross pathological changes were observed in any of the treated animals.
Repeated dose oral toxicity study in rabbit and rat : A daily single dose of Edoxaban Tosylate Monohydrate was given for 28 days to Rabbits (3/sex/group) and Wistar Rats (6/sex/group). The selected oral doses selected were 0 (Control), 1.55, 3.1 and 6.2 mg/kg bw for Rabbit and 0 (Control), 3.1, 6.2 and 12.4 mg/kg bw. In reversal groups, animals were received control and high-dose for 28 days and observed for the next 14 days. No mortality and morbidity were observed among all the groups of animals throughout the experiment period. No clinical signs were observed in any groups of the animals throughout the experiment period. No statistically significant difference in the body weight, body weight change and feed consumption of the main study group and reversal high-dose animals compared to the control group.
Reproductive toxicology : Edoxaban showed vaginal haemorrhage at higher doses in rats and rabbits but had no effects in the reproductive performance of parent rats. In rats, no effects on male or female fertility were seen.
In animal reproduction studies, rabbits showed increased incidence of gallbladder variations at a dose of 200 mg/kg which is approximately 65 times the maximum recommended human dose (MRHD) of 60 mg/day based on total body surface area in mg/m2. Increased post-implantation pregnancy losses occurred in rats at 300 mg/kg/day (approximately 49 times the MRHD) and in rabbits at 200 mg/kg/day (approximately 65 times the MRHD) respectively. Edoxaban was excreted in the breast milk of lactating rats. Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity, carcinogenic potential, or phototoxicity.
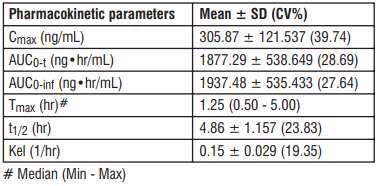
7.0 Description
Edoxaban, a factor Xa inhibitor, is supplied as Edoxaban tosylate monohydrate. The chemical name is N-(5-Chloropyridin-2-yl)- N′-[(1S,2R,4S)-4-(N, N-dimethylcarbamoyl)-2-(5-methyl-4,5,6,7-tetrahydro[1,3]thiazolo[5,4-c]pyridine-2- carboxamido)cyclohexyl] oxamide mono (4-methylbenzenesulfonate) monohydrate.
Molecular formula : C24H30ClN7O4S•C7H8O3S•H2O
Molecular weight : 738.27 g/mo
8.0 Pharmaceutical particulars
8.1 Incompatibilities
Not applicable
8.2 Shelf-life
Refer on the pack.
8.3 Packaging information
Supexa OD 15 : Alu-Alu blister strip of 15 tablets.
Supexa OD 30 : Alu-Alu blister strip of 15 tablets.
Supexa OD 60 : Alu-Alu blister strip of 15 tablets.
8.4 Storage and handling instructions
Store below 30°C. Protect from moisture.
Keep out of reach of children.
9.0 Patient counselling information
Instruct patients on the following points when administering the drug.
- Advise patients to take Supexa OD tablet exactly as prescribed.
- Remind patients to not discontinue Supexa OD tablet without talking to the healthcare provider who prescribed it.
- Instruct patients to keep an adequate supply of tablets to ensure continuous dosing of Supexa OD tablet.
- Instruct patients who cannot swallow the tablet whole to crush Supexa OD tablet, combine with 2 to 3 ounces of water or applesauce and ingest immediately.
- Instruct patients who require a gastric tube to crush the Supexa OD tablet and mix it with 2 to 3 ounces of water before administering immediately via the gastric feeding tube.
- Inform patients that if a dose is missed, they should take Supexa OD tablet as soon as possible the same day and resume the normal dosing schedule the following day. The dose should not be doubled to make up for a missing dose.
Bleeding risk
- Advise patients that they may bleed more easily, may bleed longer or bruise more easily when treated with Supexa OD tablet.
- Instruct patients to report any unusual bleeding immediately to their healthcare provider.
- For patients that are having neuraxial anesthesia or spinal puncture, advise patients to watch for signs and symptoms of spinal or epidural hematoma, such as back pain, tingling, numbness (especially in the lower limbs), muscle weakness and stool or urine incontinence. If any of these symptoms occur, advise the patient to contact his or her physician immediately.
Invasive or surgical procedures
- Remind patients to inform their healthcare providers that they are taking Supexa OD tablet before any surgery, medical or dental procedure is scheduled.
Concomitant medication and herbals
- Remind patients to inform their healthcare providers and dentists if they plan to take or are taking any prescription medications, over-the-counter drugs or herbal products.
Pregnancy
- Remind patients to inform their healthcare provider immediately if they become pregnant or intend to become pregnant during treatment with Supexa OD tablet.
- Inform patients to not breast-feed if they are taking Supexa OD tablet.
12.0 Date of issue
06 January 2025
About leaflet
Read all of this leaflet carefully before you start taking this medicine because it contains important information for you.
- Keep this leaflet. You may need to read it again.
- If you have any further questions, ask your doctor or pharmacist.
- This medicine has been prescribed for you only. Do not pass it on to others. It may harm them, even if their signs of illness are the same as yours.
- If you get any side effects, talk to your doctor or pharmacist. This includes any possible side effects not listed in this leaflet. See section 4.
What is in this leaflet
- What Supexa OD is and what it is used for
- What you need to know before you take Supexa OD
- How to take Supexa OD
- Possible side effects
- How to store Supexa OD
- Contents of the pack and other information
1. What Supexa OD is and what it is used for
Supexa OD contains the active substance edoxaban and belongs to a group of medicines called anticoagulants. This medicine helps to prevent blood clots from forming. It works by blocking the activity of factor Xa, which is an important component of blood clotting.
Supexa OD is used in adults to:
- prevent blood clots in the brain (stroke) and other blood vessels in the body if you have a form of irregular heart rhythm called nonvalvular atrial fibrillation and at least one additional risk factor, such as heart failure, previous stroke or high blood pressure;
- treat blood clots in the veins of the legs (deep vein thrombosis) and in the blood vessels in the lungs (pulmonary embolism), and to prevent blood clots from re-occurring in the blood vessels in the legs and/or lungs.
2. What you need to know before you take Supexa OD
Do not take Supexa OD
- if you are allergic to edoxaban or any of the other ingredients of this medicine
- if you are actively bleeding
- if you have a disease or condition that increases the risk of serious bleeding (e.g. stomach ulcer, injury or bleeding in the brain, or recent surgery of the brain or eyes).
- if you are taking other medicines to prevent blood clotting (e.g. warfarin, dabigatran, rivaroxaban, apixaban or heparin), except when changing anticoagulant treatment or while getting heparin through a venous or arterial line to keep it open.
- if you have a liver disease which leads to an increased risk of bleeding.
- if you have uncontrolled high blood pressure.
- if you are pregnant or breast feeding.
Warnings and precautions
Talk to your doctor or pharmacist before taking Supexa OD,
if you have an increased risk of bleeding, as could be the case if you have any of the following conditions:
- end stage kidney disease or if you are on dialysis
- severe liver disease
- bleeding disorders
- a problem with the blood vessels in the back of your eyes (retinopathy)
- recent bleeding in your brain (intracranial or intracerebral bleeding)
- problems with the blood vessels in your brain or spinal column
If you have a mechanical heart valve.
Supexa OD 15 mg is only to be used when changing from Supexa OD 30 mg to a vitamin K antagonist (e.g. warfarin).
Take special care with Supexa OD,
- if you know that you have a disease called antiphospholipid syndrome (a disorder of the immune system that causes an increased risk for blood clots), tell your doctor who will decide if the treatment may need to be changed.
If you need to have an operation
- it is very important to take Supexa OD before and after the operation exactly at the times you have been told by your doctor. If possible, Supexa OD should be stopped at least 24 hours before an operation. Your doctor will determine when to restart Supexa OD. In emergency situations your physician will help determine the appropriate actions regarding Supexa OD.
Children and adolescents
Supexa OD is not recommended in children and adolescents under 18 years of age.
Other medicines and Supexa OD
Tell your doctor or pharmacist if you are taking, have recently taken or might take any other medicines.
If you are taking any of the following:
- some medicines for fungal infections (e.g. ketoconazole);
- medicines to treat abnormal heart beat (e.g. dronedarone, quinidine, verapamil);
- other medicines to reduce blood clotting (e.g. heparin, clopidogrel or vitamin K antagonists such as warfarin, acenocoumarol, phenprocoumon or dabigatran, rivaroxaban, apixaban);
- antibiotic medicines (e.g. erythromycin, clarithromycin);
- medicines to prevent organ rejection after transplantation (e.g. ciclosporin);
- anti-inflammatory and pain-relieving medicines (e.g. naproxen or acetylsalicylic acid);
- antidepressant medicines called selective serotonin reuptake inhibitors or serotonin-norepinephrine reuptake inhibitors;
If any of the above apply to you, tell your doctor before taking Supexa OD, because these medicines may increase the effects of Supexa OD and the chance of unwanted bleeding. Your doctor will decide, if you should be treated with Supexa OD and if you should be kept under observation.
If you are taking any of the following:
- some medicines for treatment of epilepsy (e.g. phenytoin, carbamazepine, phenobarbital).
- St John’s Wort, a herbal product used for anxiety and mild depression.
- rifampicin, an antibiotic medicine.
If any of the above apply to you, tell your doctor before taking Supexa OD, because the effect of Supexa OD may be reduced. Your doctor will decide if you should be treated with Supexa OD and if you should be kept under observation.
Pregnancy and breast-feeding
Do not take Supexa OD if you are pregnant or breast-feeding. If there is a chance that you could become pregnant, use a reliable contraceptive while you are taking Supexa OD. If you become pregnant while you are taking Supexa OD, immediately tell your doctor, who will decide how you should be treated.
Driving and using machines
Supexa OD has no or negligible effects on your ability to drive or use machines.
3. How to take Supexa OD
Always take this medicine exactly as your doctor or pharmacist has told you. Check with your doctor or pharmacist if you are not sure.
How much to take?
The recommended dose is one 60 mg tablet once daily.
If you have impaired kidney function, the dose may be reduced to one 30 mg tablet once daily by your doctor.
if your body weight is 60 kg or lower, the recommended dose is one 30 mg tablet once daily;
if your doctor has prescribed medicines known as P-gp inhibitors: ciclosporin, dronedarone, erythromycin, or ketoconazole, the recommended dose is one 30 mg tablet once daily.
How to take the tablet?
Swallow the tablet, preferably with water.
Supexa OD can be taken with or without food.
If you have difficulty swallowing the tablet whole, talk to your doctor about other ways to take Supexa OD. The tablet may be crushed and mixed with water or apple puree immediately before you take it. If necessary, your doctor may also give you the crushed Supexa OD tablet through a tube via the nose (nasogastric tube) or a tube in the stomach (gastric feeding tube).
Your doctor may change your anticoagulant treatment as follows:
Changing from vitamin K antagonists (e.g. warfarin) to Supexa OD
Stop taking the vitamin K antagonist (e.g. warfarin). Your doctor will need to do blood measurements and will instruct you when to start taking Supexa OD.
Changing from non-VKA oral anticoagulants (dabigatran, rivaroxaban, or apixaban) to Supexa OD
Stop taking the previous medicines (e.g. dabigatran, rivaroxaban, or apixaban) and start Supexa OD at the time of the next scheduled dose.
Changing from parenteral anticoagulants (e.g. heparin) to Supexa OD
Stop taking the anticoagulant (e.g. heparin) and start Supexa OD at the time of the next scheduled anticoagulant dose.
Changing from Supexa OD to vitamin K antagonists (e.g. warfarin)
If you currently take 60 mg Supexa OD:
Your doctor will tell you to reduce your dose of Supexa OD to a 30 mg tablet once daily and to take it together with a vitamin K antagonist (e.g. warfarin). Your doctor will need to do blood measurements and will instruct you when to stop taking Supexa OD.
If you currently take 30 mg (dose reduced) Supexa OD:
Your doctor will tell you to reduce your dose of Supexa OD to a 15 mg tablet once daily and to take it together with a vitamin K antagonist (e.g. warfarin). Your doctor will need to do blood measurements and will instruct you when to stop taking Supexa OD.
Changing from Supexa OD to non-VKA oral anticoagulants (dabigatran, rivaroxaban, or apixaban)
Stop taking Supexa OD and start the non-VKA anticoagulant (e.g. dabigatran, rivaroxaban, or apixaban) at the time of the next scheduled dose of Supexa OD.
Changing from Supexa OD to parenteral anticoagulants (e.g. heparin)
Stop taking Supexa OD and start the parenteral anticoagulant (e.g. heparin) at the time of the next scheduled dose of Supexa OD.
Patients undergoing cardioversion:
If your abnormal heartbeat needs to be restored to normal by a procedure called cardioversion, take Supexa OD at the times your doctor tells you to prevent blood clots in the brain and other blood vessels in your body.
If you take more Supexa OD than you should
Tell your doctor immediately if you have taken too many Supexa OD tablets.
If you take more Supexa OD than recommended, you may have an increased risk of bleeding.
If you forget to take Supexa OD
You should take the tablet immediately and then continue the following day with the once daily tablet as usual. Do not take a double dose on the same day to make up for a forgotten dose.
If you stop taking Supexa OD
Do not stop taking Supexa OD without talking to your doctor first, because Supexa OD treats and prevents serious conditions.
If you have any further questions on the use of this medicine, ask your doctor or pharmacist.
4. Possible side effects
Like all medicines, this medicine can cause side effects, although not everybody gets them. Like other similar medicines (medicines to reduce blood clotting), Supexa OD may cause bleeding which may potentially be life-threatening. In some cases, the bleeding may not be obvious.
If you experience any bleeding event that does not stop by itself or if you experience signs of excessive bleeding (exceptional weakness, tiredness, paleness, dizziness, headache or unexplained swelling) consult your doctor immediately.
Your doctor may decide to keep you under closer observation or change your medicine.
Overall list of possible side effects:
Common (may affect up to 1 in 10 people)
- stomach ache
- abnormal liver blood tests
- bleeding from the skin or under the skin
- anaemia (low levels of red blood cells)
- bleeding from the nose
- bleeding from the vagina
- rash
- bleeding in the bowel
- bleeding from the mouth and/or throat
- blood found in your urine
- bleeding following an injury (puncture)
- bleeding in the stomach
- dizziness
- feeling sick
- headache
- itching
Uncommon (may affect up to 1 in 100 people)
- bleeding in the eyes
- bleeding from a surgical wound following an operation
- blood in the spit when coughing
- bleeding in the brain
- other types of bleeding
- reduced number of platelets in your blood (which can affect clotting)
- allergic reaction
- hives
Rare (may affect up to 1 in 1,000 people)
- bleeding in the muscles
- bleeding in joints
- bleeding in the abdomen
- bleeding in the heart
- bleeding inside the skull
- bleeding following a surgical procedure
- allergic shock
- swelling of any part of the body due to allergic reaction
Not known (frequency cannot be estimated from the available data)
- bleeding in the kidney sometimes with presence of blood in urine leading to inability of the kidneys to work properly (anticoagulant-related nephropathy).
Reporting of side effects
If you get any side effects, talk to your doctor, pharmacist or nurse. This includes any possible side effects not listed in this leaflet. You can also report side effects directly: Website: www.zuventus.com and click the tab “Safety Reporting” located on the top end of the home page. Website link: https://www.zuventus.com/drug-safety-reporting
By reporting side effects, you can help provide more information on the safety of this medicine. You can also report the side effect with the help of your treating physician.
5. How to store Supexa OD
Keep this medicine out of the sight and reach of children.
Do not use this medicine after the expiry date which is stated on the carton and on each blister or bottle after EXP. The expiry date refers to the last day of that month.
This medicine does not require any special storage conditions.
Do not throw away any medicines via wastewater or household waste. Ask your pharmacist how to throw away medicines you no longer use. These measures will help protect the environment.
6. Contents of the pack and other information
What Supexa OD contains
- The active substance is edoxaban (as tosylate monohydrate).
Supexa OD 15 mg film-coated tablets
Each tablet contains 15 mg edoxaban (as tosylate monohydrate).
Supexa OD 30 mg film-coated tablets
Each tablet contains 30 mg edoxaban (as tosylate monohydrate).
Supexa OD 60 mg film-coated tablets
Each tablet contains 60 mg edoxaban (as tosylate monohydrate).