Zensita D 100 Tablets









Therapy Area
Anti-diabetic
1.0 Generic Name
Sitagliptin and Dapagliflozin Tablets
2.0 Qualitative and quantitative composition
Zensita-D 50/5
Each film coated tablet contains :
Sitagliptin Phosphate Monohydrate IP equivalent to Sitagliptin 50 mg
Dapagliflozin Propanediol Monohydrate equivalent to Dapagliflozin 5 mg
Excipients q.s.
Colours : Titanium Dioxide IP & Ferric Oxide Red USP NF
Zensita-D 100/10
Each film coated tablet contains :
Sitagliptin Phosphate Monohydrate IP equivalent to Sitagliptin 100 mg
Dapagliflozin Propanediol Monohydrate equivalent to Dapagliflozin 10 mg
Excipients q.s.
Colours : Titanium Dioxide IP & Ferric Oxide Red USP NF
3.0 Dosage form and strength
Film coated tablet
4.0 Clinical Particulars
4.1 Therapeutic Indication
Sitagliptin and Dapagliflozin are indicated for the treatment of type 2 diabetes mellitus inadequately controlled on Metformin monotherapy.
4.2 Posology & Method of Administration
The dosage of Sitagliptin and Dapagliflozin should be individualized on the basis of the patient's current regimen, effectiveness, and tolerability while not exceeding the maximum recommended daily dose of 100 mg Sitagliptin and 10 mg Dapagliflozin. Initial combination therapy or maintenance of combination therapy should be individualized and left to the discretion of the health care provider.
Method of administration
Sitagliptin and Dapagliflozin can be taken with or without food.
4.3 Contraindications
Sitagliptin and Dapagliflozin is contraindicated in patients with: Sitagliptin Patients with a history of a hypersensitive reaction to Sitagliptin or to any ingredient in the formulation. Prohibited Medications Strong CYP2C8 inhibitors (e.g., Gemfibrozil), CYP2C8 inducers (e.g., Rifampin) and Topiramate. Drugs increasing hypoglycemic action: β-blocking agents, Salicylic acid and Monoamine oxidase inhibitor. Drugs decreasing hypoglycemic action: Adrenalin and adrenocortical hormone. Drugs known to cause QT prolongation: Class IA antiarrhythmic drug Quinidine sulfate hydrate, Procainamide Hydrochloride, Class III antiarrhythmic drugs Amiodarone Hydrochloride, Sotalol Hydrochloride. Digoxin and Oral hypoglycemic agents other than study medication. Diuretics, Insulin and insulin secretagogues, such as sulphonylureas, Rifampicin and Mefenamic Acid. Oral hypoglycemic agents other than study medication.
Dapagliflozin
• Patients with a history of hypersensitivity reaction to the active substance or to any of the excipients.
• Patients with an estimated glomerular filtration rate (eGFR) less than 45 mL/min/1.73 m , severe renal impairment, end-stage renal disease (ESRD) or patients on dialysis
4.4 Warning & Precautions
Volume depletion: Before initiating Sitagliptin and Dapagliflozin, assess volume status and renal function in the elderly, patients with renal impairment or low systolic blood pressure, and in patients on diuretics. Monitor for signs and symptoms during therapy. Ketoacidosis in Patients with Diabetes Mellitus: Assess patients who present with signs and symptoms of metabolic acidosis for ketoacidosis regardless of blood glucose level. If suspected, discontinue Sitagliptin and Dapagliflozin, evaluate and treat promptly. Before initiating Sitagliptin and Dapagliflozin, consider risk factors for ketoacidosis. Patients on Sitagliptin and Dapagliflozin may require monitoring and temporary discontinuation of therapy in clinical situations known to predispose to ketoacidosis. Urosepsis and Pyelonephritis: Evaluate for signs and symptoms of urinary tract infections and treat promptly, if indicated.
Hypoglycemia: Consider a lower dose of insulin or the insulin secretagogue to reduce the risk of hypoglycemia when used in combination with Sitagliptin and Dapagliflozin. Necrotizing Fasciitis of the Perineum (Fournier's Gangrene): Serious, life-threatening cases have occurred in patients with diabetes, both females and males. Assess patients presenting with pain or tenderness, erythema, or swelling in the genital or perineal area, along with fever or malaise. If suspected, institute prompt treatment.
Genital Mycotic Infections: Monitor and treat if indicated. There have been post marketing reports of acute pancreatitis, including fatal and non-fatal haemorrhagic or necrotizing pancreatitis. If pancreatitis is suspected, promptly discontinue Sitagliptin and Dapagliflozin. There have been post marketing reports of acute renal failure, sometimes requiring dialysis. Dosage adjustment is recommended in patients with moderate or severe renal insufficiency and in patients with ESRD. Assessment of renal function is recommended prior to initiating Sitagliptin and Dapagliflozin and periodically thereafter. There is an increased risk of hypoglycaemia when Sitagliptin and Dapagliflozin is added to an insulin secretagogue (e.g., sulfonylurea) or insulin therapy. Consider lowering the dose of the sulfonylurea or insulin to reduce the risk of hypoglycemia. There have been post marketing reports of serious allergic and hypersensitivity reactions in patients treated with Sitagliptin and Dapagliflozin such as anaphylaxis, angioedema, and exfoliative skin conditions including Steven Johnson syndrome. In such cases, promptly stop Sitagliptin and Dapagliflozin, assess for other potential causes, institute appropriate monitoring and treatment, and initiate alternative treatment for diabetes. There have been no clinical studies establishing conclusive evidence of macro vascular risk reduction with Sitagliptin and Dapagliflozin or any other anti-diabetic drug
4.5 Drug Interactions
Digoxin
There was a slight increase in the area under the curve (AUC, 11%) and mean peak drug concentration (C , 18%) of digoxin with the co-administration of 100 mg sitagliptin for 10 days. Patients receiving max digoxin should be monitored appropriately. No dosage adjustment of digoxin or Sitagliptin and Dapagliflozin is recommended. Positive Urine Glucose Test Monitoring glycemic control with urine glucose tests is not recommended in patients taking SGLT2 inhibitors as SGLT2 inhibitors increase urinary glucose excretion and will lead to positive urine glucose tests. Use alternative methods to monitor glycemic control. Interference with 1,5-anhydroglucitol (1,5-AG) Assay Monitoring glycemic control with 1,5-AG assay is not recommended as measurements of 1,5-AG are unreliable in assessing glycemic control in patients taking SGLT2 inhibitors. Use alternative methods to monitor glycemic control.
4.6 Special populations
Pregnancy
There are no adequate and well-controlled studies in pregnant women with Sitagliptin and Dapagliflozin or its individual components; therefore, the safety of Sitagliptin and Dapagliflozin in pregnant women is not known.
Sitagliptin and Dapagliflozin should be used during pregnancy only if clearly needed. Reproduction studies have been performed in rats and rabbits. Doses of sitagliptin up to 125 mg/kg (approximately 12 times the human exposure at the maximum recommended human dose) did not impair fertility or harm the foetus.
The data are based on findings in studies performed with Sitagliptin and Dapagliflozin individually
Nursing woman
No studies in lactating animals have been conducted with the combined components of Sitagliptin and Dapagliflozin.
In studies performed with the individual components, both Sitagliptin and Dapagliflozin are secreted in the milk of lactating rats. It is not known whether sitagliptin is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when Sitagliptin and Dapagliflozin is administered to a nursing woman.
Paediatric Use
Safety and effectiveness of Sitagliptin and Dapagliflozin in paediatric patients under 18 years have not been established.
Geriatric Use
No Sitagliptin and Dapagliflozin dosage change is recommended based on age.
4.7 Effects on ability to drive and use machines
Sitagliptin and Dapagliflozin has no or negligible influence on the ability to drive and use machines.
4.8 Undesirable Effects
Undesirable Effects Adverse reactions reported in 5% of patients treated with Sitagliptin and more commonly than in patients treated with placebo are: upper respiratory tract infection, nasopharyngitis and headache. In the add on to sulfonylurea and add-on to insulin studies, hypoglycemia was also more commonly reported in patients treated with Dapagliflozin compared to placebo. The most common adverse reactions associated with Dapagliflozin (5% or greater incidence) were female genital mycotic infections, nasopharyngitis, and urinary tract infection. Arthralgia ADR is reported with sitagliptin
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via email to: medico@zuventus.com Website: http://www.zuventus.co.in/safety.aspx
By reporting side effects, you can help provide more information on the safety of this medicine.
4.9 Overdose
Sitagliptin
During controlled clinical trials in healthy subjects, single doses of up to 800 mg Sitagliptin were administered.
Maximal mean increases in QTc of 8.0 msec were observed in one study at a dose of 800 mg Sitagliptin, a mean effect that is not considered clinically important. There is no experience with doses above 800 mg in clinical studies. In Phase I multiple-dose studies, there were no dose-related clinical adverse reactions observed with Sitagliptin with doses of up to 600 mg per day for periods of up to 10 days and 400 mg per day for up to 28 days. In the event of an overdose, it is reasonable to employ the usual supportive measures, e.g., remove unabsorbed material from the gastrointestinal tract, employ clinical monitoring (including obtaining an electrocardiogram), and institute supportive therapy as dictated by the patient's clinical status. Sitagliptin is modestly dialyzable. In clinical studies, approximately 13.5% of the dose was removed over a 3- to 4- hour haemodialysis session. Prolonged haemodialysis may be considered if clinically appropriate. It is not known if sitagliptin is dialyzable by peritoneal dialysis.
Dapagliflozin
There were no reports of overdose during the clinical development program for dapagliflozin. In the event of an overdose, contact the Poison Control Centre. It is also reasonable to employ supportive measures as dictated by the patient's clinical status. The removal of dapagliflozin by haemodialysis has not been studied.
5.0 Pharmacological properties
5.1 Mechanism of Action
Sitagliptin and Dapagliflozin combines two antihyperglycemic agents with complementary mechanisms of action to improve glycemic control in patients with type 2 diabetes: sitagliptin, a dipeptidyl peptidase-4 (DPP-4) inhibitor, and metformin hydrochloride, a member of the biguanide class. Sitagliptin and Dapagliflozin are indicated for the treatment of type 2 diabetes mellitus inadequately controlled on Metformin monotherapy.
Dapagliflozin
Sodium-glucose cotransporter 2 (SGLT2), expressed in the proximal renal tubules, is responsible for the majority of the reabsorption of filtered glucose from the tubular lumen. Dapagliflozin is an inhibitor of SGLT2. By inhibiting SGLT2, dapagliflozin reduces reabsorption of filtered glucose and lowers the renal threshold for glucose, and thereby increases urinary glucose excretion. Dapagliflozin also reduces sodium reabsorption and increases the delivery of sodium to the distal tubule. This may influence several physiological functions including, but not restricted to, lowering both pre- and afterload of the heart and downregulation of sympathetic activity.
Sitagliptin
Sitagliptin is a DPP-4 inhibitor, which is believed to exert its actions in patients with type 2 diabetes by slowing the inactivation of incretin hormones. Concentrations of the active intact hormones are increased by sitagliptin, thereby increasing and prolonging the action of these hormones. Incretin hormones, including glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP), are released by the intestine throughout the day, and levels are increased in response to a meal. These hormones are rapidly inactivated by the enzyme DPP-4. The incretins are part of an endogenous system involved in the physiologic regulation of glucose homeostasis. When blood glucose concentrations are normal or elevated, GLP-1 and GIP increase insulin synthesis and release from pancreatic beta cells by intracellular signalling pathways involving cyclic AMP. GLP-1 also lowers glucagon secretion from pancreatic alpha cells, leading to reduced hepatic glucose production. By increasing and prolonging active incretin levels, sitagliptin increases insulin release and decreases glucagon levels in the circulation in a glucosedependent manner. Sitagliptin demonstrates selectivity for DPP-4 and does not inhibit DPP-8 or DPP-9 activity in vitro at concentrations approximating those from therapeutic doses.
5.2 Pharmacodynamic Properties
Dapagliflozin
Increases in the amount of glucose excreted in the urine were observed in healthy subjects and in patients with type 2 diabetes mellitus following the administration of dapagliflozin. Dapagliflozin doses of 5 or 10 mg per day in patients with type 2 diabetes mellitus for 12 weeks resulted in excretion of approximately 70 grams of glucose in the urine per day at Week 12. A near maximum glucose excretion was observed at the dapagliflozin daily dose of 20 mg. This urinary glucose excretion with dapagliflozin also results in increases in urinary volume. After discontinuation of dapagliflozin, on average, the elevation in urinary glucose excretion approaches baseline by about 3 days for the 10 mg dose.
Sitagliptin
General
In patients with type 2 diabetes, administration of sitagliptin led to inhibition of DPP-4 enzyme activity for a 24-hour period. After an oral glucose load or a meal, this DPP-4 inhibition resulted in a 2- to 3-fold increase in circulating levels of active GLP-1 and GIP, decreased glucagon concentrations, and increased responsiveness of insulin release to glucose, resulting in higher C-peptide and insulin concentrations. The rise in insulin with the decrease in glucagon was associated with lower fasting glucose concentrations and reduced glucose excursion following an oral glucose load or a meal. In studies with healthy subjects, sitagliptin did not lower blood glucose or cause hypoglycemia.
Cardiac Electrophysiology In a randomized, placebo-controlled crossover study, 79 healthy subjects were administered a single oral dose of sitagliptin 100 mg, sitagliptin 800 mg (8 times the recommended dose), and placebo. At the recommended dose of 100 mg, there was no effect on the QTc interval obtained at the peak plasma concentration, or at any other time during the study. Following the 800-mg dose, the maximum increase in the placebo-corrected mean change in QTc from baseline at 3 hours post dose was 8.0 msec. This increase is not considered to be clinically significant. At the 800-mg dose, peak sitagliptin plasma concentrations were approximately 11 times higher than the peak concentrations following a 100-mg dose. In patients with type 2 diabetes administered sitagliptin 100 mg (N=81) or sitagliptin 200 mg (N=63) daily, there were no meaningful changes in QTc interval based on ECG data obtained at the time of expected peak plasma concentration.
5.3 Pharmacokinetic properties
Absorption
Sitagliptin
The absolute bioavailability of sitagliptin is approximately 87%. Co-administration of a high-fat meal with sitagliptin had no effect on the pharmacokinetics of sitagliptin
Dapagliflozin
Following oral administration of dapagliflozin, the maximum plasma concentration (C ) is usually max attained within 2 hours under fasting state. The C and AUC values increase dose proportionally with max increase in dapagliflozin dose in the therapeutic dose range. The absolute oral bioavailability of dapagliflozin following the administration of a 10 mg dose is 78%. Administration of dapagliflozin with a high-fat meal decreases its C by up to 50% and prolongs T by approximately 1 hour, but does not alter max max AUC as compared with the fasted state. These changes are not considered to be clinically meaningful and dapagliflozin can be administered with or without food.
Distribution
Sitagliptin
The mean volume of distribution at steady state following a single 100-mg intravenous dose of sitagliptin to healthy subjects is approximately 198 litres. The fraction of sitagliptin reversibly bound to plasma proteins is low (38%).
Dapagliflozin
Dapagliflozin is approximately 91% protein bound. Protein binding is not altered in patients with renal or hepatic impairment.
Biotransformation
Sitagliptin
Sitagliptin is primarily eliminated unchanged in urine, and metabolism is a minor pathway. Approximately 79 % of sitagliptin is excreted unchanged in the urine. Following a sitagliptin oral dose, approximately 16 % of the radioactivity was excreted as metabolites of sitagliptin. Six metabolites were detected at trace levels and are not expected to contribute to the plasma DPP-4 inhibitory activity of sitagliptin. In vitro studies indicated that the primary enzyme responsible for the limited metabolism of sitagliptin was CYP3A4, with contribution from CYP2C8. In vitro data showed that sitagliptin is not an inhibitor of CYP isozymes CYP3A4, 2C8, 2C9, 2D6, 1A2, 2C19 or 2B6, and is not an inducer of CYP3A4 and CYP1A2.
Dapagliflozin
Dapagliflozin is approximately 91% protein bound. Protein binding is not altered in patients with renal or hepatic impairment.
Elimination
Sitagliptin
Following administration of an oral sitagliptin dose to healthy subjects, approximately 100 % of the administered radioactivity was eliminated in faeces (13 %) or urine (87 %) within one week of dosing. The apparent terminal t following a 100-mg oral dose of sitagliptin was approximately 12.4 hours. Sitagliptin accumulates only minimally with multiple doses. The renal clearance was approximately 350 mL/min. Elimination of sitagliptin occurs primarily via renal excretion and involves active tubular secretion. Sitagliptin is a substrate for human organic anion transporter-3 (hOAT-3), which may be involved in the renal elimination of sitagliptin. The clinical relevance of hOAT-3 in sitagliptin transport has not been established. Sitagliptin is also a substrate of p-glycoprotein, which may also be involved in mediating the renal elimination of sitagliptin. However, ciclosporin, a p-glycoprotein inhibitor, did not reduce the renal clearance of sitagliptin. Sitagliptin is not a substrate for OCT2 or OAT1 or PEPT1/2 transporters. In vitro, sitagliptin did not inhibit OAT3 (IC50=160 μM) or p-glycoprotein (up to 250 μM) mediated transport at therapeutically relevant plasma concentrations. In a clinical study sitagliptin had a small effect on plasma digoxin concentrations indicating that sitagliptin may be a mild inhibitor of p-glycoprotein.
Dapagliflozin
Dapagliflozin and related metabolites are primarily eliminated via the renal pathway. Following a single 14 50 mg dose of [ C]-dapagliflozin, 75% and 21% total radioactivity is excreted in urine and faces, respectively. In urine, less than 2% of the dose is excreted as parent drug. In faces, approximately 15% of the dose is excreted as parent drug. The mean plasma terminal half-life (t½) for dapagliflozin is approximately 12.9 hours following a single oral dose of Dapagliflozin 10 mg.
Special populations
Renal Insufficiency
Sitagliptin
An approximately 2-fold increase in the plasma AUC of sitagliptin was observed in patients with moderate renal insufficiency, and an approximately 4-fold increase was observed in patients with severe renal insufficiency including patients with ESRD on haemodialysis, as compared to normal healthy control subjects
Dapagliflozin
At steady-state (20 mg once daily dapagliflozin for 7 days), patients with type 2 diabetes with mild, moderate, or severe renal impairment (as determined by eGFR) had geometric mean systemic exposures of dapagliflozin that were 45%, 2.04-fold, and 3.03-fold higher, respectively, as compared to patients with type 2 diabetes mellitus with normal renal function. Higher systemic exposure of dapagliflozin in patients with type 2 diabetes mellitus with renal impairment did not result in a correspondingly higher 24-hour urinary glucose excretion. The steady-state 24-hour urinary glucose excretion in patients with type 2 diabetes mellitus and mild, moderate, and severe renal impairment was 42%, 80%, and 90% lower, respectively, than in patients with type 2 diabetes mellitus with normal renal function. The impact of haemodialysis on dapagliflozin exposure is not known.
Hepatic Insufficiency
Sitagliptin
In patients with moderate hepatic insufficiency (Child-Pugh score 7 to 9), mean AUC and C of sitagliptin max increased approximately 21% and 13%, respectively, compared to healthy matched controls following administration of a single 100-mg dose of sitagliptin. These differences are not considered to be clinically meaningful. There is no clinical experience in patients with severe hepatic insufficiency (Child-Pugh score >9).
Dapagliflozin
In subjects with mild and moderate hepatic impairment (Child-Pugh classes A and B), mean C and AUC max of dapagliflozin were up to 12% and 36% higher, respectively, as compared to healthy matched control subjects following single-dose administration of 10 mg dapagliflozin. These differences were not considered to be clinically meaningful. In patients with severe hepatic impairment (Child-Pugh class C), mean Cmax and AUC of dapagliflozin were up to 40% and 67% higher, respectively, as compared to healthy max matched controls
Gender
Sitagliptin
Gender had no clinically meaningful effect on the pharmacokinetics of sitagliptin based on a composite analysis of Phase I pharmacokinetic data and on a population pharmacokinetic analysis of Phase I and Phase II data.
Geriatric
Sitagliptin
When the effects of age on renal function are taken into account, age alone did not have a clinically meaningful impact on the pharmacokinetics of sitagliptin based on a population pharmacokinetic analysis
Elderly subjects (65 to 80 years) had approximately 19% higher plasma concentrations of sitagliptin compared to younger subjects.
Dapagliflozin
Based on a population pharmacokinetic analysis, age, gender, race, and body weight do not have a clinically meaningful effect on the pharmacokinetics of dapagliflozin and thus, no dose adjustment is recommended.
Paediatric
Sitagliptin
Race had no clinically meaningful effect on the pharmacokinetics of sitagliptin based on a composite analysis of available pharmacokinetic data, including subjects of white, Hispanic, black, Asian, and other racial groups.
Dapagliflozin
Pharmacokinetics in the paediatric population has not been studied.
6.0 Nonclinical properties
6.1 Animal Toxicology or Pharmacology
No animal studies have been conducted with the combined products in Sitagliptin and Dapagliflozin to evaluate effects. Sitagliptin reproduction studies have been performed in rats and rabbits. Doses of sitagliptin up to 125 mg/kg (approximately 12 times the human exposure at the maximum recommended human dose) did not impair fertility or harm the foetus. There are, however, no adequate and wellcontrolled studies with sitagliptin in pregnant women. Sitagliptin administered to pregnant female rats and rabbits from gestation day 6 to 20 (organogenesis) was not teratogenic at oral doses up to 250 mg/kg (rats) and 125 mg/kg (rabbits), or approximately 30 and 20 times human exposure at the maximum recommended human dose (MRHD) of 100 mg/day based on AUC comparisons. Higher doses increased the incidence of rib malformations in offspring at 1000 mg/kg, or approximately 100 times human exposure at the MRHD. Sitagliptin administered to female rats from gestation day 6 to lactation day 21 decreased body weight in male and female offspring at 1000 mg/kg. No functional or behavioural toxicity was observed in offspring of rats. Placental transfer of sitagliptin administered to pregnant rats was approximately 45% at 2 hours and 80% at 24 hours post dose. Placental transfer of sitagliptin administered to pregnant rabbits was approximately 66% at 2 hours and 30% at 24 hours.
7.0 Description
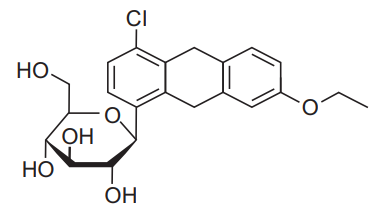
Dapagliflozin
Dapagliflozin is described chemically as D-glucitol, 1,5-anhydro-1-C-[4-chloro-3-[(4 ethoxyphenyl) methyl]phenyl]-, (1S)-, compounded with (2S)-1,2-propanediol, hydrate (1:1:1). The empirical formula is C21H25ClO6C8H8O2H2O and the molecular weight is 502.98. The structural formula is
Sitagliptin
Sitagliptin is an orally-active inhibitor of the dipeptidyl peptidase-4 (DPP-4) enzyme. Sitagliptin is present in the form of sitagliptin phosphate monohydrate. Sitagliptin phosphate monohydrate is described chemically as 7-[(3R)-3- amino-1-oxo-4-(2,4,5-trifluorophenyl)butyl]-5,6,7,8tetrahydro-3- (trifluoromethyl)- 1,2,4- triazolo[4,3-a]pyrazine phosphate (1:1) monohydrate with an empirical formula of C16H15F6N5O•H3PO4 •H2O and a molecular weight of 523.32. The structural formula is:
8.0 List of excipients:
Core Tablet:
Microcrystalline Cellulose
Croscarmellose sodium
PVP K 30
Purified water*
Croscarmellose sodium
Colloidal silicon dioxide
Mannitol
Magnesium Stearate
Film Coating:
Polyvinyl Alcohol
Polyethylene Glycol
Talc
Titanium Dioxide
Ferric Oxide Red
9.0 Pharmaceutical particulars
9.1 Incompatibilities
Not Applicable
9.2 Shelf Life
Refer on the pack.
9.3 Packaging Information
Alu-Alu blister strip of 10 tablets.
9.4 Storage and handing Instructions
Store below 30°C. Protect from light.
Keep out of reach of children.
10.0 Patient counselling information
What is the most important information I should know about Sitagliptin and Dapagliflozin Tablets?
• Patients with a history of hypersensitivity reaction to the active substance or to any of the excipients.
• Patients with an estimated glomerular filtration rate (eGFR) less than 45 mL/min/1.73 m2, severe renal impairment, end-stage renal disease (ESRD) or patients on dialysis
Sitagliptin
Patients with a history of a hypersensitive reaction to Sitagliptin or to any ingredient in the formulation. Prohibited Medications
Strong CYP2C8 inhibitors (e.g., Gemfibrozil), CYP2C8 inducers (e.g., Rifampin) and Topiramate. Drugs increasing hypoglycemic action: β-blocking agents, Salicylic acid and Monoamine oxidase inhibitor. Drugs decreasing hypoglycemic action: Adrenalin and adrenocortical hormone. Drugs known to cause QT prolongation: Class IA antiarrhythmic drug Quinidine sulfate hydrate, Procainamide Hydrochloride, Class III antiarrhythmic drugs
Amiodarone Hydrochloride, Sotalol Hydrochloride. Digoxin and Oral hypoglycemic agents other than study medication. Diuretics, Insulin and insulin secretagogues, such as sulphonylureas, Rifampicin and Mefenamic Acid. Oral hypoglycemic agents other than study medication. Call your doctor right away if you have any of the following symptoms, which could be signs of lactic acidosis:
• you feel cold in your hands or feet
• you feel dizzy or lightheaded
• you have a slow or irregular heartbeat
• you feel very weak or tired
• you have unusual (not normal) muscle pain
• you have trouble breathing
• you feel sleepy or drowsy
• you have stomach pains, nausea or vomiting
Do not take Sitagliptin and Dapagliflozin Tablets:
If you are allergic to Sitagliptin and Dapagliflozin or any of the other ingredients of this medicine. If you think you may be allergic to Sitagliptin and Dapagliflozin or any of the other ingredients of Sitagliptin and Dapagliflozin, do not take this medicine and talk to your doctor.
Warnings and precautions
Talk to your doctor, pharmacist or nurse before taking Sitagliptin and Dapagliflozin. If you take Sitagliptin and Dapagliflozin with another medicine that can cause low blood sugar, such as a sulfonylurea or insulin, your risk of getting low blood sugar is higher. The dose of your sulfonylurea medicine or insulin may need to be lowered while you use Sitagliptin and Dapagliflozin. Signs and symptoms of may include:
• Upper respiratory tract infection,
• Nasopharyngitis
• Headache
• Hypoglycemia
• Female genital mycotic infections
What is type 2 diabetes?
Type 2 diabetes is a condition in which your body does not make enough insulin, and the insulin that your body produces does not work as well as it should. Your body can also make too much sugar. When this happens, sugar (glucose) builds up in the blood. This can lead to serious medical problems. High blood sugar can be lowered by diet and exercise, and by certain medicines when necessary
How will I receive Sitagliptin and Dapagliflozin Tablets?
Swallow the tablets whole with some water.
If you take more Sitagliptin and Dapagliflozin Tablets than you should?
If you have taken too many tablets, contact your doctor immediately or go to the nearest hospital casualty department taking any remaining medication and this patient information leaflet with you.
If you forget to take Sitagliptin and Dapagliflozin Tablets?
If you miss a dose of Sitagliptin and Dapagliflozin Tablets, take it as soon as possible. However, if it is almost time for your next dose, skip the missed dose and go back to your regular schedule. Do not double the dose.
About Leaflet
Read all of this leaflet carefully before you start taking this medicine because it contains important information for you.
- Keep this leaflet. You may need to read it again.
- If you have any further questions, ask your doctor, pharmacist or nurse.
- This medicine has been prescribed for you only. Do not pass it on to others. It may harm them, even if their signs of illness are the same as yours.
- If you get any side effects, talk to your doctor or pharmacist. This includes any possible side effects not listed in this leaflet. See section 4.
What is in this leaflet:
- What Zensita-D is and what it is used for
- What you need to know before you take Zensita-D
- How to take Zensita-D
- Possible side effects
- How to store Zensita-D
- Contents of the pack and other information
1. What Zensita-D is and what it is used for
Zensita-D contains the active substances sitagliptin and dapagliflozin. Each belongs to a group of medicines called “oral anti-diabetics”. These medicines are taken by mouth for diabetes.
Sitagliptin and Dapagliflozin are indicated for the treatment of type 2 diabetes mellitus inadequately controlled on Metformin monotherapy.
If you have type 2 diabetes, your pancreas does not make enough insulin or your body is not able to use the insulin it produces properly. This leads to a high level of sugar in your blood.
Zensita-D is used to treat type 2 diabetes when:
- sitagliptin or dapagliflozin alone, together with metformin and/or sulphonylurea cannot control your diabetes.
- you are already being treated with sitagliptin and dapagliflozin as single tablets. Your doctor may ask you to switch to this medicine.
- It is important to continue to follow the advice on diet and exercise given to you by your doctor, pharmacist or nurse.
2. What you need to know before you take Zensita-D
Do not take Zensita-D:
- if you are allergic to sitagliptin, dapagliflozin or any of the other ingredients of this medicine (listed in section 6).
- if you have had a serious allergic reaction to any other similar medicines (for example DPP-4 inhibitors like sitagliptin, linagliptin, alogliptin, or SGLT2 inhibitors like canagliflozin, empagliflozin) that you take to control your blood sugar.
Do not take Zensita-D if any of the above apply to you. If you are not sure, talk to your doctor, pharmacist, or nurse before taking this medicine.
Warnings and precautions
Talk to your doctor, pharmacist or nurse before taking Zensita-D, and during treatment:
- if you have or have had a disease of the pancreas called pancreatitis. Possible signs of pancreatitis are listed in section 4.
- if you are on medicines to lower your blood pressure (anti-hypertensives) and have a history of low blood pressure (hypotension).
- For more information, see section “Other medicines and Zensita-D” below. if you have very high levels of sugar in your blood which may make you dehydrated (lose too much body fluid).
- Possible signs of dehydration are listed at the top of section 4. Tell your doctor before you start taking Zensita-D if you have any of these signs.
- if you have or develop nausea (feeling sick), vomiting or fever or if you are not able to eat or drink. These conditions can cause dehydration.
- Your doctor may ask you to stop taking Zensita-D until you recover to prevent dehydration.
- if you have moderate or severe liver problem.
- if you experience rapid weight loss, feeling sick or being sick, stomach pain, excessive thirst, fast and deep breathing, confusion, unusual sleepiness or tiredness, a sweet smell to your breath, a sweet or metallic taste in your mouth, or a different odour to your urine or sweat, contact a doctor or the nearest hospital straight away. These symptoms could be a sign of “diabetic ketoacidosis” – a rare but serious, sometimes life-threatening problem you can get with diabetes because of increased levels of “ketone bodies” in your urine or blood, seen in tests. The risk of developing diabetic ketoacidosis may be increased with prolonged fasting, excessive alcohol consumption, dehydration, sudden reductions in insulin dose, or a higher need of insulin due to major surgery or serious illness.
- if you have “type 1 diabetes” your body does not produce any insulin. Zensita-D should not be used to treat this condition.
- if you have or have had a serious hypersensitivity (allergic) reaction or is suspected. Signs of a serious allergic reaction are listed in section 4. if you often get infections of the urinary tract.
- if you have a history of serious heart disease. if you suffer from heart failure or you have other risk factors for developing heart failure such as problems with your kidneys. Your doctor will advise you of the signs and symptoms of heart failure.
- Symptoms can include, but are not limited to, increasing shortness of breath, rapid increase in weight and swelling of the feet (pedal oedema). You should call your doctor, pharmacist or nurse immediately if you experience any of these symptoms. if you have severe joint pain.
- if your body’s ability to fight infections is reduced, for example if you have a disease like AIDS or have undergone an organ transplant. if you are taking a medicine to lower your blood sugar, such as sulphonylureas (see “Other medicines and Zensita-D”). If any of the above apply to you (or you are not sure), talk to your doctor, pharmacist or nurse before taking Zensita-D.
- Diabetic skin lesions (skin damage such as sores or ulcers) are a common complication of diabetes. Rash has been seen with both sitagliptin and dapagliflozin when given separately (see section 4). You are advised to follow the recommendations for skin care that you are given by your doctor or nurse. Contact your doctor if you encounter blistering of the skin, as it may be a sign for a condition called bullous pemphigoid. Your doctor may ask you to stop Zensita-D.
- Like for all diabetic patients it is important to check your feet regularly and adhere to any other advice regarding foot care given by your health care professional. Talk to your doctor immediately if you develop a combination of symptoms of pain, tenderness, redness, or swelling of the genitals or the area between the genitals and the anus with fever or feeling generally unwell.
- These symptoms could be a sign of a rare but serious or even life-threatening infection, called necrotising fasciitis of the perineum or Fournier’s gangrene which destroys the tissue under the skin. Fournier’s gangrene has to be treated immediately.
Kidney function
- Your kidneys should be checked before you start taking Zensita-D. During treatment with this medicine, your doctor will check your kidney function once a year or more frequently if you have worsening kidney function.
Urine tests
- Because of how Zensita-D works, your urine will test positive for sugar while you are on this medicine.
Children and adolescents
- Zensita-D is not recommended for children and adolescents under 18 years of age, because it has not been studied in these patients.
Other medicines and Zensita-D
- Tell your doctor, pharmacist or nurse if you are taking, have recently taken or might take any other medicines.
Especially tell your doctor:
- if you are taking a medicine used to increase the amount of water you pass out of the body (diuretic). Your doctor may ask you to stop taking Zensita-D. Possible signs of losing too much fluid from your body are listed at the top of section 4.
- if you are taking another medicine that lowers the amount of sugar in your blood such as a sulphonylurea (for example glimepiride). Your doctor may want to lower the dose of this other medicine, to prevent you from getting low blood sugar levels (hypoglycaemia).
- if you are using medicines containing any of the following active substances, that might have an effect on the breakdown of Zensita-D in your body. Your doctor may ask you to check your blood sugar levels more often while taking these medicines.
- Carbamazepine, phenobarbital or phenytoin. These may be used to control fits (seizures) or chronic pain.
- Dexamethasone – a steroid medicine. This may be used to treat inflammation in different body parts and organs.
- Rifampicin. This is an antibiotic used to treat infections such as tuberculosis.
- Ketoconazole. This may be used to treat fungal infections. Diltiazem.
- This is a medicine used to treat angina (chest pain) and lower blood pressure. If any of the above apply to you (or if you are not sure), talk to your doctor before taking Zensita-D.
Pregnancy and breast-feeding
If you are pregnant or breast-feeding, think you may be pregnant or are planning to have a baby, ask your doctor or pharmacist for advice before taking this medicine. Zensita-D is not recommended during pregnancy and your doctor will ask you to stop taking this medicine if you become pregnant. Talk to your doctor about the best way to control your blood sugar while you are pregnant.
You should not use Zensita-D if you are breast-feeding. It is not known if this medicine passes into human breast milk. Talk to your doctor if you would like to or are breast-feeding before taking this medicine.
Driving and using machines
Zensita-D is not expected to affect you being able to drive a car or use any tools or machines. If you feel dizzy while taking this medicine, do not drive or use any tools or machines. Taking this medicine together with another medicine that lowers your blood sugar, such as a sulphonylurea, can cause too low blood sugar levels (hypoglycaemia). This may cause symptoms such as shaking, sweating and change in vision, and may affect your ability to drive and use machines.
Zensita-D contains lactose
Zensita-D contains lactose (milk sugar). If you have been told by your doctor that you have an intolerance to some sugars, contact your doctor before taking this medicine.
Zensita-D contains sodium
Zensita-D contains less than 1 mmol sodium (23 mg) per dose, that is to say essentially ‘sodium free’.
3. How to take Zensita-D
Always take this medicine exactly as your doctor has told you. Check with your doctor, pharmacist or nurse if you are not sure.
How much to take
• The recommended dose is one tablet once or twice daily.
The dosage of Sitagliptin and Dapagliflozin should be individualized on the basis of the patient's current regimen, effectiveness, and tolerability while not exceeding the maximum recommended daily dose of 100 mg Sitagliptin and 10 mg Dapagliflozin. Initial combination therapy or maintenance of combination therapy should be individualized and left to the discretion of the health care provider.
Taking this medicine
- Swallow the tablet whole with half a glass of water.
- You can take your tablet with or without food.
- You can take the tablet at any time of the day. However, try to take it at the same time each day. This will help you to remember to take it.
Your doctor may prescribe other medicines to lower the amount of sugar in your blood.
Remember to take other medicine(s) as your doctor has told you. This will help get the best results for your health.
Diet and exercise
To control your diabetes, you still need to keep to diet and exercise, even when you are taking this medicine. So it is important to keep following the advice about diet and exercise from your doctor, pharmacist or nurse. In particular, if you are following a diabetic weight control diet, continue to follow it while you are taking Zensita-D.
If you take more Zensita-D than you should
If you take more Zensita-D tablets than you should, talk to a doctor or go to a hospital straight away. Take the medicine pack with you.
If you forget to take Zensita-D
What to do if you forget to take a tablet.
- If it is less than 12 hours since you should have taken your dose, take a dose of Zensita-D as soon as you remember. Then take your next dose at the usual time.
- If it is more than 12 hours since you should have taken your dose, skip the missed dose.
- Then take your next dose at the usual time.
- Do not take a double dose of Zensita-D to make up for a forgotten dose. If you stop taking Zensita-D
Do not stop taking Zensita-D without talking to your doctor first. Your blood sugar may increase without this medicine.
If you have any further questions on the use of this medicine, ask your doctor, pharmacist or nurse.
4. Possible side effects
Like all medicines, this medicine can cause side effects, although not everybody gets them.
Stop taking Zensita-D and see a doctor straight away if you notice any of the following serious side effects:
• Symptoms of a serious allergic reaction (anaphylactic reaction, angioedema) seen rarely, (may affect up to 1 in 1 000 people), which may include:
- rash,
- raised red patches on your skin (hives), swelling of the face,
- lips,
- tongue,
- and throat that may cause difficulty in breathing or swallowing.
- Your doctor may prescribe a medicine to treat your allergic reaction and a different medicine for your diabetes.
Pancreatitis, seen uncommonly (may affect up to 1 in 100 people): severe and persistent pain in the abdomen (stomach area) which might reach through to your back, as well as nausea and vomiting, as it could be a sign of an inflamed pancreas.
Dehydration, (loss of too much fluid from your body), seen uncommonly.
These are signs of dehydration:
- very dry or sticky mouth, feeling very thirsty,
- feeling very sleepy or tired,
- passing little or no water (urine),
- fast heartbeat.
• Urinary tract infection, seen commonly (may affect up to 1 in 10 people).
These are signs of a severe infection of the urinary tract:
- fever and/or chills,
- burning sensation when passing water (urinating),
- pain in your back or side.
Although uncommon, if you see blood in your urine, tell your doctor immediately.
• Low blood sugar levels (hypoglycaemia), seen very commonly (may affect more than 1 in 10 people) if used with other diabetes medicines known to cause hypoglycaemia.
These are the signs of low blood sugar:
- shaking, sweating, feeling very anxious, fast heart beat,
- feeling hungry, headache, change in vision,
- a change in your mood or feeling confused.
Your doctor will tell you how to treat low blood sugar levels and what to do if you get any of the signs above.
• Diabetic ketoacidosis, seen rarely.
These are the signs of diabetic ketoacidosis (see also section 2 Warnings and precautions):
- increased levels of “ketone bodies” in your urine or blood,
- rapid weight loss,
- feeling sick or being sick,
- stomach pain,
- excessive thirst,
- fast and deep breathing,
- confusion,
- unusual sleepiness or tiredness,
- a sweet smell to your breath, a sweet or metallic taste in your mouth or a different odour to your urine or sweat.
This may occur regardless of blood glucose level. Your doctor may decide to temporarily or permanently stop your treatment with Zensita-D.
• Necrotising fasciitis of the perineum or Fournier’s gangrene, a serious soft tissue infection of the genitals or the area between the genitals and the anus, seen very rarely (may affect up to 1 in 10 000 people).
Stop taking Zensita-D and see a doctor or nurse straight away, if you notice any of the serious side effects above.
Other side effects when taking Zensita-D alone or in combination with metformin:
Very common
- upper respiratory tract infection including:
- infection of the upper chest or lungs,
- infection of the sinuses with a feeling of pain and fullness behind your cheeks and eyes (sinusitis),
- inflamed nose or throat (nasopharyngitis) (signs of this may include a cold or a sore throat).
Common
• genital infection (thrush) of your penis or vagina (signs may include irritation, itching, unusual discharge or odour)
• back pain
• passing more water (urine) than usual or needing to pass water more often
• changes in the amount of cholesterol or fats in your blood (shown in tests)
• increases in the amount of red blood cells in your blood (shown in tests)
• decreases in creatinine renal clearance (shown in tests) in the beginning of treatment
• dizziness
• tiredness
• severe joint pain (arthralgia)
• stomach ache and indigestion (dyspepsia)
• nausea
• diarrhoea
• inflamed stomach or gut usually caused by an infection (gastroenteritis)
• headache, muscle pain (myalgia)
• vomiting, inflammation of the stomach (gastritis)
• rash
Uncommon
• thirst • constipation
• awakening from sleep at night to pass urine
• dry mouth
• weight decreased
• increases in creatinine (shown in laboratory blood tests) in the beginning of treatment
• increases in urea (shown in laboratory blood tests)
• skin rash that may include raised bumps, skin irritation, or unpleasant itchiness
• difficulties in getting or maintaining an erection (erectile dysfunction)
• fungal infection
• hypersensitivity reactions
• itching in the genital area (pruritus genital or vulvovaginal pruritus) or discomfort while urinating
Not known (frequency cannot be estimated from the available data)
• blistering of the skin (bullous pemphigoid)
Reporting of side effects
If you get any side effects, talk to your doctor. This includes any possible side effects not listed in this leaflet. You can also report side effects directly: Website: www.zuventus.co.in and click the tab “Safety Reporting” located on the top of the home page.
By reporting side effects, you can help provide more information on the safety of this medicine.
5. How to store Zensita-D
Keep this medicine out of the sight and reach of children.
Do not use this medicine after the expiry date, which is stated on the blister and carton after ‘EXP’. The expiry date refers to the last day of that month.
This medicine does not require any special storage conditions.
Do not throw away any medicines via wastewater or household waste. Ask your pharmacist how to throw away medicines you no longer use. These measures will help to protect the environment.
6. Contents of the pack and other information
What Zensita-D contains
• The active substances are sitagliptin and dapagliflozin.
• Each tablet contains sitagliptin+ dapagliflozin (50+5) mg / (100+10) mg. 10 Blister strips of 10 tablets each