4.1 Therapeutic indication
For the treatment of severe opioid responsive pain conditions which are not adequately responding to nonopioid analgesics.
4.2 Posology and method of administration
Bupreplast patch should be administered every 7th day. Bupreplast patch is not suitable for the treatment of acute pain.
Patients aged 18 years and over
The lowest Bupreplast patch dose (Bupreplast 5 mcg/hr transdermal patch) should be used as the initial dose. Consideration should be given to the previous opioid history of the patient as well as to the current general condition and medical status of the patient.
Titration
During initiation and titration with Bupreplast, patients should use the usual recommended doses of short acting supplemental analgesics as needed until analgesic efficacy with Bupreplast patch is attained. The dose should not be increased before 3 days, when the maximum effect of a given dose is established. Subsequent dosage increases may then be titrated based on the need for supplemental pain relief and the patient's analgesic response to the patch.
To increase the dose, a larger patch should replace the patch that is currently being worn, or a combination of patches should be applied in different places to achieve the desired dose. It is recommended that no more than two patches are applied at the same time, regardless of the patch strength. A new patch should not be applied to the same skin site for the subsequent 3-4 weeks. Patients should be carefully and regularly monitored to assess the optimum dose and duration of treatment.
Conversion from opioids
Patch can be used as an alternative to treatment with other opioids. Such patients should be started on the lowest available dose (Bupreplast 5 mcg/hr transdermal patch) and continue taking short-acting supplemental analgesics during titration as required.
Patients under 18 years of age
As buprenorphine patch has not been studied in patients under 18 years of age,the use of Bupreplast patch in patients below this age is not recommended.
Elderly
No dosage adjustment of Bupreplast patch is required in elderly patients.
Renal impairment
No special dose adjustment of Bupreplast patch is necessary in patients with renal impairment.
Hepatic impairment
Buprenorphine is metabolised in the liver. The intensity and duration of its action may be affected in patients with impaired liver function. Therefore patients with hepatic insufficiency should be carefully monitored during treatment with Bupreplast patch. Patients with severe hepatic impairment may accumulate buprenorphine during Bupreplast patch treatment. Consideration of alternate therapy should be considered, and Bupreplast should be used with caution, if at all, in such patients.
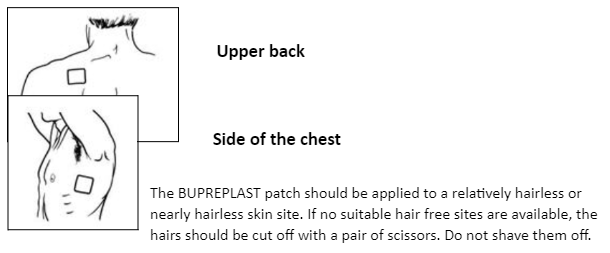
Patch application
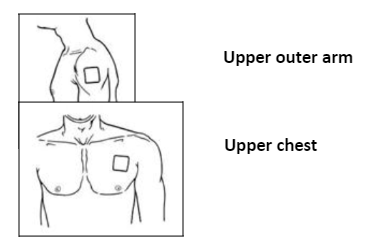
Bupreplast should be applied to non-lrritated, Intact skin of the upper outer arm, upper chest, upper back or side of the chest, but not to any parts of the skin with large scars. Bupreplast patch should be applied to a relatively hairless or nearly hairless skin site. If none are available, the hair at the site should be cut with scissors, not shaven.
If the application site must be cleaned, It should be done with clean water only. Soaps, alcohol, oil, lotions of abrasive devices must not be used. The skin must be dry before the patch is applied. Bupreplast should be applied immediately after removal from the sealed sachet. Following removal of the protective layer, the transdermal patch should be pressed firmly in place with the palm of the hand for approximately 30 seconds, making sure the contact is complete, especially around the edges. If the edges of the patch begin to peel off, the edges may be taped down with suitable skin tape.
The patch should be worn continuously for 7 days.
Bathing, showering, or swimming should not affect the patch. If a patch falls off, a new one should be applied.
Duration of administration
Bupreplast should under no circumstances be administered for longer than absolutely necessary. If long-term pain treatment with Bupreplast is necessary in view of the nature and severity to the illness, then careful and regular monitoring should be carried out (If necessary with breaks in treatment) to establish whether and to what extent further treatment is necessary.
Discontinuation
After removal of the patch, buprenorphine serum concentrations decrease gradually and thus the analgesic effect is maintained for a certain amount of time. This should be considered when therapy with Bupreplast is to be followed by other opioids. As a general rule, a subsequent opioid should not be administered within 24 hours after removal of the patch. At present, only limited information is available on the starting dose of other opioids administered after discontinuation of the transdermal patch.
Patients with fever or exposed to external heat
While wearing the patch, patients should be advised to avoid exposing the application site to external heat sources, such as heating pads, electric blankets, heat lamps, sauna, hot tubs, and heated water beds, etc., as an increase in absorption of buprenorphine may occur. When treating febrile patients, one should be aware that fever may also increase absorption resulting in increased plasma concentrations of buprenorphine and thereby increased risk of opioid reactions.
4.3 Contraindications
Buprenorphine patch is contraindicated in :
- Patients with known hypersensitivity to the active substance buprenorphine or to any of the excipients.
- The treatment of opioid dependence and narcotic withdrawal.
- Conditions in which the respiratory centre and function are severely impaired or may become so.
- Patients who are receiving MAO inhibitors or have taken them within the last two weeks.
- Patients suffering from myasthenia gravis
- Patients suffering from delirium tremens
- Pregnancy (see "Warnings & Precautions").
4.4 Special warnings and precautions for use
- Buprenorphine should be used with particular caution in patients with acute alcohol intoxication, head injury, shock, a reduced level of consciousness of uncertain origin, intracranial lesions or increased intracranial pressure, or in patients with severe hepatic impairment.
- Buprenorphine may lower the seizure threshold in patients with a history of seizure disorder.
- Significant respiratory depression has been associated with buprenorphine, particularly by the intravenous route. A number of overdose deaths have occurred when addicts have intravenously abused buprenorphine, usually with benzodiazepines concomitantly. Additional overdose deaths due to ethanol and benzodiazepines in combination with buprenorphine have been reported.
- Since CYP3A4 inhibitors may increase concentrations of buprenorphine, patients already treated with CYP3A4 inhibitors should have their dose of Buprenorphine carefully titrated since a reduced dosage might be sufficient in these patients.
- Buprenorphine is not recommended for analgesia in the immediate post-operative period or in other situations characterised by a narrow therapeutic index or a rapidly varying analgesic requirement.
- Controlled human and animal studies indicate that buprenorphine has a lower dependence liability than pure agonist analgesics. In humans limited euphorigenic effects have been observed with buprenorphine. This may result in some abuse of the medicinal product and caution should be exercised when prescribing to patients known to have, or suspected of having, a history of drug abuse or alcohol abuse or serious mental illness.
- As with all opioids chronic use of buprenorphine can result in the development of physical dependence. Withdrawal (abstinence syndrome), when it occurs, is generally mild, begins after 2 days and may last up to 2 weeks. Withdrawal symptoms include agitation, anxiety, nervousness, insomnia, hyperkinesia, tremor and gastrointestinal disorders.
- Athletes should be aware that this medicine may cause a positive reaction to sports doping control tests.
- Risk from concomitant use of sedative medicines such as benzodiazepines or related drugs : Concomitant use of Buprenorphine and sedative medicines such as benzodiazepines or related drugs may result in sedation, respiratory depression, coma and death. Because of these risks, concomitant prescribing with these sedative medicines should be reserved for patients for whom alternative treatment options are not possible. If a decision is made to prescribe Buprenorphine concomitantly with sedative medicines, the lowest effective dose should be used, and the duration of treatment should be as short as possible.
- The patients should be followed closely for signs and symptoms of respiratory depression and sedation. In this respect, it is strongly recommended to inform patients and their caregivers to be aware of these symptoms.
Serotonin syndrome
Concomitant administration of Buprenorphine and other serotonergic agents, such as MAO inhibitors, selective serotonin re-uptake inhibitors (SSRIs), serotonin norepinephrine re-uptake inhibitors (SNRIs) or tricyclic antidepressants may result in serotonin syndrome, a potentially life-threatening condition.
If concomitant treatment with other serotonergic agents is clinically warranted, careful observation of the patient is advised, particularly during treatment initiation and dose increases.
Symptoms of serotonin syndrome may include mental-status changes, autonomic instability, neuromuscular abnormalities, and/or gastrointestinal symptoms.
If serotonin syndrome is suspected, a dose reduction or discontinuation of therapy should be considered depending on the severity of the symptoms.
4.5 Drugs interactions
Buprenorphine must not be used concomitantly with MAOIs or in patients who have received MAOIs within the previous two weeks. Effect of other active substances on the pharmacokinetics of buprenorphine :
- Buprenorphine is primarily metabolised by glucuronidation and to a lesser extent (about 30%) by CYP3A4.
- Concomitant treatment with CYP3A4 inhibitors may lead to elevated plasma concentrations with intensified efficacy of buprenorphine.
- Studies with the CYP3A4 inhibitor ketoconazole did not produce clinically relevant increases in mean maximum (Cmax) or total (AUC) buprenorphine exposure following buprenorphine with ketoconazole as compared to buprenorphine alone.
- The interaction between buprenorphine and CYP3A4 enzyme inducers has not been studied.
- Co-administration of buprenorphine and enzyme inducers (e.g. phenobarbital, carbamazepine, phenytoin and rifampicin) could lead to increased clearance which might result in reduced efficacy.
- Reductions in hepatic blood flow induced by some general anaesthetics (e.g. halothane) and other medicinal products may result in a decreased rate of hepatic elimination of buprenorphine.
Pharmacodynamic interactions
Buprenorphine should be used cautiously with :
- Other central nervous system depressants : other opioid derivatives (analgesics and antitussives containing e.g. morphine, dextropro-poxyphene, codeine, dextromethorphan or noscapine). Certain anti-depressants, sedative H1-receptor antagonists, alcohol, anxiolytics, neuroleptics, clonidine and related substances. These combinations increase the CNS depressant activity. Benzodiazepines : This combination can potentiate respiratory depression of central origin.
- At typical analgesic doses buprenorphine is described to function as a pure mu receptor agonist. In buprenorphine clinical studies subjects receiving full mu agonist opioids (up to 90 mg oral morphine or oral morphine equivalents per day) were transferred to buprenorphine. There were no reports of abstinence syndrome or opioid withdrawal during conversion from entry opioid to buprenorphine.
- Sedative medicines such as benzodiazepines or related drugs The concomitant use of opioids with sedative medicines such as benzodiazepines or related drugs increases the risk of sedation, respiratory depression, coma and death because of additive CNS depressant effect. The dose and duration of concomitant use should be limited Co-administration of Serotonergic medicinal products, such as MAO inhibitors, selective serotonin re-uptake inhibitors (SSRIs), serotonin norepinephrine re-uptake inhibitors (SNRIs) or tricyclic antidepressants as the risk of serotonin syndrome, a potentially life-threatening condition, is increased.
4.6 Use in special populations
Pregnancy
There are no or limited amount of data from the use of buprenorphine in pregnant women. Studies in animals have shown reproductive toxicity. The potential risk for humans is unknown. Towards the end of pregnancy high doses of buprenorphine may induce respiratory depression in the neonate even after a short period of administration. Prolonged use of buprenorphine during pregnancy can result in neonatal opioid withdrawal. Therefore, buprenorphine should not be used during pregnancy and in women of childbearing potential who are not using effective contraception.
Nursing Mothers
Buprenorphine is excreted in human milk. Studies in rats have shown that buprenorphine may inhibit lactation. Available pharmacodynamic / toxicological data in animals has shown excretion of buprenorphine in milk. Therefore, the use of buprenorphine during lactation should be avoided.
Fertility
No human data on the effect of buprenorphine on fertility are available. In a fertility and early embryonic development study, no effects on reproductive parameters were observed in male or female rats
4.7 Effects on ability to drive and use machines
Buprenorphine has major influence on the ability to drive and use machines. Even when used according to instructions, buprenorphine patch may affect the patient's reactions to such an extent that road safety and the ability to operate machinery may be impaired. This applies particularly in the beginning of treatment and in conjunction with other centrally acting substances including alcohol, tranquillisers, sedatives and hypnotics. An individual recommendation should be given by the physician. A general restriction is not necessary in cases where a stable
dose is used.
In patients who are affected, such as during treatment initiation or titration to a higher dose, these patients should not drive or use machines, nor for at least 24 hours after the patch has been removed.
This medicine can impair cognitive function and can affect a patient's ability to drive safely. When prescribing this medicine, patients should be told :
- The medicine is likely to affect your ability to drive.
- Do not drive until you know how the medicine affects you.
4.8 Undesirable effects
Serious adverse reactions that may be associated with buprenorphine patch therapy in clinical use are similar to those observed with other opioid analgesics, including respiratory depression (especially when used with other CNS depressants) and hypotension. The following undesirable effects have occurred :
Very common (> 1/10, common (> 1/100, <1/10, uncommon (>/1000, < 1/100), rare (> 1/10,000 < 1/1000), very rare (< 1/10,000 including isolated reports).
Immune system disorders
Uncommon : hypersensitivity
Very rare : anaphylactic reaction, anaphylactoid reaction
Metabolism and nutrition disorders
Common : anorexia
Uncommon : dehydration
Psychiatric disorders
Common : confusion, depression, insomnia, nervousness
Uncommon : sleep disorder, restlessness, agitation, depersonalization, euphoric mood, affect lability, anxiety, hallucinations, nightmares
Rare : psychotic disorder, decreased libido
Very rare : drug dependence, mood swings
Nervous system disorders
Very common : headache, dizziness, somnolence Common: paresthesia Uncommon : sedation, dysgeusia, dysarthria, hypoaesthesia, memory impairment, migraine, syncope, tremor, abnormal coordination, disturbance in attention
Rare : balance disorder, speech disorder Very rare: involuntary muscle contractions
Eye disorders
Uncommon : dry eye, blurred vision
Rare : visual disturbance, eyelid oedema, miosis
Ear and labyrinth disorders
Uncommon : tinnitus, vertigo
Very rare : ear pain
Cardiac disorders
Uncommon : angina pectoris, palpitations, tachycardia
Vascular disorders
Common : vasodilation
Uncommon : hypotension, circulatory collapse, hypertension, flushing
Respiratory, thoracic and mediastinal disorders
Common : dyspnoea
Uncommon : asthma aggravated, cough, hypoxia, rhinitis, wheezing, hyperventilation, hiccups Rare: respirator y depression, respirator y failure
Gastrointestinal disorders
Very common : constipation, dry mouth, nausea, vomiting
Common : abdominal pain, diarrhoea, dyspepsia
Uncommon : flatulence
Rare : diverticulitis, dysphagia, ileus
Hepatobiliary disorders
Rare : Biliary colic
Skin and subcutaneous tissue disorders
Very common : pruritus, erythema
Common : rash, sweating, exanthema
Uncommon : dry skin, face oedema, urticaria Very rare : pustules, vesicles
Musculoskeletal and connective tissue disorders
Uncommon : Muscle cramp, myalgia, muscular weakness, muscle spasms
Renal and urinary disorders
Uncommon : urinary retention, micturition disorders
Reproductive system and breast disorders
Rare : erectile dysfunction, sexual dysfunction
General disorders and administration site conditions
Very common : application site pruritus, application site reaction
Common : tiredness, asthenia pain, peripheral oedema, application site reaction, erythema at site, rash at site, oedema, chest pain
Uncommon : fatigue, influenza like illness, pyrexia, rigors, malaise, oedema, drug withdrawal syndrome
Rare : application site inflammation
Investigations
Uncommon : alanine aminotransferase increased, weight decreased
Injury, poisoning and procedural complications
Uncommon : Accidental injury fall
* In some cases delayed local allergic reactions occurred with marked signs of inflammation. In such cases treatment with buprenorphine patch should be terminated.
Buprenorphine has a low risk of physical dependence. After discontinuation of buprenorphine patch, withdrawal symptoms are unlikely. This may be due to the very slow dissociation of buprenorphine from the opioid receptors and to the gradual decrease of buprenorphine plasma concentrations (usually over a period of 30 hours after removal of the last patch). However, after long-term use of buprenorphine patch, withdrawal symptoms similar to those occurring during opioid withdrawal, cannot be entirely excluded. These symptoms include agitation, anxiety, nervousness, insomnia, hyperkinesia tremor and gastrointestinal disorders.
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit / risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via email to :medico@zuventus.com
Website : https://www.zuventus.com/drug-safety-reporting
Very common : headache, dizziness, somnolence Common: paresthesia Uncommon : sedation, dysgeusia, dysarthria, hypoaesthesia, memory impairment, migraine, syncope, tremor, abnormal coordination, disturbance in attention Rare : balance disorder, speech disorder Very rare: involuntary muscle contractions
4.9 Overdose
Symptoms : Symptoms similar to those of other centrally acting analgesics are to be expected. These include respiratory depression, sedation, drowsiness, nausea, vomiting, cardiovascular collapse and marked miosis.
Treatment : Remove any patches from the patient's skin. Establish and maintain a patent airway, assist or control respiration as indicated and maintain adequate body temperature and fluid balance. Oxygen, intravenous fluids, vasopressors and other supportive measures should be employed as indicated.
A specific opioid antagonist such as naloxone may reverse the effects of buprenorphine. The dose of naloxone may be in the range 5 to 12 mg intravenously.