Mr. Sanjay Rajanikant Mehta is a Non-executive Director of the Company. He is a graduate in Commerce from the Pune University. He has been associated with pharma industry for more than two decades. He is on the Board of the Company since 2006.
C Tax-OF Tablets
1.0 Generic name
Cefixime & Ofloxacin Tablets
2.0 Qualitative and quantitative composition
Each film coated tablet contains:
Cefixime (as Trihydrate) IP equivalent to Anhydrous Cefixime 200 mg
Ofloxacin IP 200 mg
Excipients q.s.
Colours: Lake of Quinoline Yellow & Titanium Dioxide IP
3.0 Dosage form and strength
Film coated tablet
Cefixime (200mg) and Ofloxacin (200mg)
4.0 Clinical particulars
4.1 Therapeutic Indication
For the treatment of patients with typhoid fever and urinary tract infection in adults.
4.2 Posology and method of administration
C Tax-OF adult dose:
1 tablet two times daily.
4.3 Contraindications
- Persons with a history of hypersensitivity associated with the use of ofloxacin or any member of the quinolone group. Patients with known allergy to cefixime or other cephalosporins.
- Patients with a past history of tendinitis related to fluoroquinolone administration.
- Patients with a history of epilepsy or seizures.
- Children or growing adolescents and in pregnant or breast-feeding women, since animal experiments do not entirely exclude the risk of damage to the cartilage of joints in the growing subject
- Patients with latent or actual defects in G6PD activity
4.4 Special warnings and precautions for use
The drug may cause low blood sugar and mental health related side effects. Low blood sugar levels, also called hypoglycaemia, can lead to coma. The mental health side effects more prominent and more consistent across the systemic fluoroquinolone drug class. The mental health side effects to be added to or updated across all the fluoroquinolones are:
- Disturbances in attention
- Disorientation
- Agitation
- Nervousness
- Memory impairment
- Serious disturbances in mental abilities called delirium
| Condition | Description |
| Hypersensitivity and allergic reactions | Hypersensitivity, severe cutaneous ADRs such as TEN, Stevens-Johnson syndrome and drug rash with eosinophilia and systemic symptoms (DRESS) have been reported in some patients. C Tax-OF should be discontinued and appropriate measures should be taken |
| Hypersensitivity to penicillins | As with other cephalosporins, C Tax-OF should be given with caution to patients with a history of hypersensitivity to penicillin, as there is some evidence of cross-allergenicity |
| Hemolytic anaemia | Drug-induced hemolytic anaemia has been seen with cephalosporins (as a class) |
| Renal impairment | It should be used with caution in patients with impaired renal function |
| G6PD deficiency | Patients with G6PD may be predisposed to hemolytic reactions if they are treated with quinolones. Therefore, if C Tax-OF has to be used in these patients, potential occurrence of haemolysis should be monitored |
| Impaired liver function | C Tax-OF should be used with caution in patients with impaired liver function |
| Myasthenia gravis | C Tax-OF is not recommended in patients with a known history of myasthenia gravis |
| Photosensitization | It is recommended that patients should not expose themselves unnecessarily to strong sunlight or to artificial UV rays, during treatment and for 48 hours following treatment discontinuation |
| Superinfection | The prolonged use of C Tax-OF may result in overgrowth of non-susceptible organisms |
| Peripheral neuropathy | C Tax-OF should be discontinued if the patient experiences symptoms of neuropathy |
4.5 Drugs interactions
- Drugs known to prolong QT interval: C Tax-OF should be used with caution in patients receiving drugs known to prolong the QT interval (e.g. anti-arrhythmics, tricyclic antidepressants, macrolides, and antipsychotics).
- Antacids, Sucralfate, Metal Cations: Co-administered magnesium/aluminium antacids, sucralfate, zinc or iron preparations can reduce absorption. Therefore, ofloxacin should be taken 2 hours before such preparations.
- Theophylline, fenbufen or similar NSAIDs: A pronounced lowering of the cerebral seizure threshold may occur when quinolones are given concurrently with theophylline, NSAIDs, or other agents, which lower the seizure threshold. In case of seizures, treatment with C Tax-OF should be discontinued.
- Glibenclamide: Ofloxacin may cause a slight increase in serum concentrations of glibenclamide.
- Probenecid, cimetidine, furosemide and methotrexate: Caution should be exercised when ofloxacin is co-administered with drugs that affect the tubular renal secretion such as probenecid, cimetidine, furosemide and methotrexate.
- Vitamin K antagonists & Anticoagulants: Increased coagulation tests (PT/INR) and/or bleeding have been reported in patients treated with ofloxacin in combination with a vitamin K antagonist (e.g. warfarin). Coagulation tests should be monitored in patients treated with Vitamin-K antagonists. Cefixime should be administered with caution to patients receiving coumarin-type anticoagulants, e.g. warfarin.
- Other forms of interaction: A false positive direct coombs test has been reported during treatment with cephalosporin antibiotics, therefore it should be recognised that a positive coombs test may be due to the drug.
4.6 Use in special populations
Pregnancy
C Tax-OF should not be used during pregnancy.
Lactation
Breast feeding should be discontinued during treatment with C Tax-OF because of the potential for arthropathy and other serious toxicity in the nursing infants.
Children
C Tax-OF is not indicated for use in children or growing adolescents.
4.7 Effects on ability to drive and use machines
There have been occasional reports of drowsiness/somnolence, impairment of skills, dizziness/vertigo and visual disturbances, which may impair the patient's ability to concentrate and react, and therefore may constitute a risk in situations where these abilities are of special importance (e.g. driving a car or operating machinery), patients should know how they react to ofloxacin before they drive or operate machinery. These effects may be enhanced by alcohol.
In the case of side effects such as encephalopathy (which may include convulsion, confusion, impairment of consciousness, movement disorders), the patient should not operate machines or drive a vehicle.
4.8 Undesirable effects
Cefixime:
- Acute generalized exanthematous pustulosis and Mouth Ulceration has been reported with Cefixime use.
- The most commonly seen adverse reactions reported were gastrointestinal events (30%) in adult patients
- Individual adverse reactions included Diarrhea-16%, Loose or frequent stools- 6%, Abdominal pain-3%, Nausea-7%, Dyspepsia-3%, Flatulence 4%
Ofloxacin:
- Stevens-Johnson syndrome (SJS)/ Toxic epidermal necrolysis (TEN) has been reported with Ofloxacin use.
- The most frequently reported adverse events were nausea- 10%, headache- 9%, insomnia- 7%, external genital pruritus in women- 6%, Dizziness-5%, Vaginitis-5%, Diarrhea-4%, Vomiting 4%
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product.
Healthcare professionals are asked to report any suspected adverse reactions via email to: medico@zuventus.com
Website: https://www.zuventus.com/drug-safety-reporting
By reporting side effects, you can help provide more information on the safety of this medicine.
4.9 Overdose
Ofloxacin
Important signs of acute over dosage: CNS symptoms such as confusion, dizziness, impairment of consciousness and seizures, increases QT interval, GIT reactions e.g. nausea and mucosal erosions.
In the case of overdose steps to remove any unabsorbed ofloxacin e.g. gastric lavage, administration of adsorbants and sodium sulphate are recommended; antacids are recommended for protection of the gastric mucosa. A fraction of ofloxacin may be removed from the body with haemodialysis.
No specific antidote exists. Elimination of ofloxacin may be increased by forced diuresis. In the event of overdose, symptomatic treatment should be implemented. ECG monitoring should be undertaken, because of the possibility of QT interval prolongation.
Cefixime There is no experience with overdoses with Cefixime. Cefixime is not removed from the circulation in significant quantities by dialysis. No specific antidote exists. General supportive measures are recommended.
5.0 Pharmacological properties
5.1 Pharmacodynamic Properties
Cefixime
- is an oral third generation cephalosporin which has marked in vitro bactericidal activity against a wide variety of Gram-positive and Gram-negative organisms. Bactericidal action of cefixime results from inhibition of cell-wall synthesis.
- Active against most isolates of the following bacteria both in vitro and in clinical infections:
- Gram-positive bacteria- Streptococcus pneumonia, Streptococcus pyogenes
- Gram-negative bacteria - Haemophilus influenza, Moraxella catarrhalis, Escherichia coli, Proteus mirabilis, Neisseria gonorrhoeae
- In vitro bactericidal activity is seen against isolates of the following microorganisms.
- Gram-positive bacteria- Streptococcus agalactiae
- Gram-negative bacteria- Haemophilus parainfluenzae, Proteus vulgaris, Klebsiella pneumonia, Klebsiella oxytoca, Pasteurella multocida, Providencia species, Salmonella species, Shigella species, Citrobacter amalonaticus, Citrobacter diversus, Serratia marcescens
Ofloxacin
- Is a quinolone-carboxylic acid derivative with a wide range of antibacterial activity against both gram negative and gram positive organisms.
- The primary mode of action of the quinolones is the specific inhibition of bacterial DNA gyrase. This enzyme is required for DNA replication, transcription, repair and recombination. Its inhibition leads to expansion and destabilisation of the bacterial DNA and hence to cell death.
- Active against most isolates of the following bacteria both in vitro and in clinical infections.
- Gram-Positive Microorganisms- Staphylococcus aureus (methicillin-susceptible strains), Streptococcus pneumoniae (penicillin-susceptible), Streptococcus pyogenes
- Gram-Negative Microorganisms- Citrobacter koseri, Enterobacter aerogenes, Escherichia coli, Haemophilus influenza, Klebsiella pneumonia, Neisseria gonorrhoeae, Proteus mirabilis, Pseudomonas aeruginosa,
- Other Microorganisms- Chlamydia trachomatis
- In vitro bactericidal activity is seen against isolates of the following microorganisms
- Gram-positive microorganisms- Staphylococcus epidermidis (methicillin-susceptible strains), Staphylococcus saprophyticu, Streptococcus pneumonia,
- Gram-Negative Microorganisms- Acinetobacter calcoaceticus, Bordetella pertussis, Pasteurella multocida, Enterobacter cloacae, Haemophilus ducreyi, Klebsiella oxytoca, Moraxella catarrhalis, M. morganii, Proteus vulgaris, Providencia rettgeri, P. stuartii, Serratia marcescens
- Other microorganisms- Chlamydia pneumoniae, Gardnerella vaginalis, Legionella pneumophila, Mycoplasma pneumoniae, Ureaplasma urealyticum,
- Anaerobic Microorganisms- Clostridium perfringes
5.2 Pharmacokinetic properties
| Parameter | Cefixime | Ofloxacin |
| Oral bioavailability | 40% to 50% | Approximately 98% |
| Tmax | 2 and 5 hours | 1 to 2 hours |
| Cmax | 2 mcg/mL (range 1 to 4 mcg/mL) | 2.2 mcg/mL |
| Plasma protein binding | Approx. 65%. | Approx. 32% |
| AUC | 34.9 ± 12.2 to 49.5 ± 19.1 mg.h/L | 14.1 mcg.h/mL |
| Half life | Averages 3 to 4 hours but may range up to 9 hours in some healthy volunteers. | Biphasic elimination. Following multiple oral doses at steady-state administration, the half-lives are approximately 4 to 5 hours and 20 to 25 hours. However, the longer half-life represents less than 5% of the total AUC. Accumulation at steady-state can be estimated using a half-life of 9 hours |
| Elimination | Approx. 50% of the absorbed dose is cefixime is also excreted in the bile in excess of 10% of the administered dose. | Mainly by renal excretion |
| Renal impairment | In severe renal impairment (CrCl- 5 to 20 ml/min), the half-life increased to an average of 11.5 hrs. | Dosage adjustment is necessary for elderly and patients with impaired renal function. |
6.0 Nonclinical properties
6.1 Animal Toxicology or Pharmacology
Preclinical effects in conventional studies of safety pharmacology, acute toxicity, repeated dose toxicity, reproductive studies were observed only at exposures considered sufficiently in excess of the maximum human exposure indicating little relevance to clinical use. Joint toxicity was observed at exposure in the human therapeutic range in juvenile rats and dogs. Ofloxacin exhibits a neurotoxic potential and causes reversible testicular alterations at high doses.
Mutagenicity studies showed no evidence for mutagenicity of ofloxacin. However, like some other quinolones Ofloxacin is phototoxic in animals at exposure in the human therapeutic range. The phototoxic, photomutagenic and photocarcinogenic potential of ofloxacin is comparable with that of other gyrase inhibitors.
Preclinical data from conventional genotoxicity studies reveal no special hazard to humans, carcinogen potential has not been investigated.
Reproduction toxicity
Ofloxacin has no effect on fertility, peri- or postnatal development, and therapeutic doses did not lead to any teratogenic or other embryotoxic effects in animals. Ofloxacin crosses the placenta and levels reached in the amniotic fluid are about 30% of the maximal concentrations measured in maternal serum.
7.0 Description
Cefixime is a semisynthetic, cephalosporin antibacterial for oral administration. Ofloxacin tablets are a synthetic broad-spectrum antimicrobial agent for oral administration.
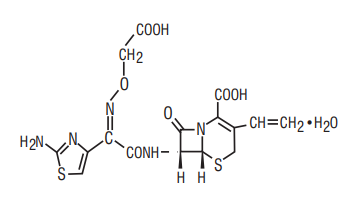
Cefixime
Chemical Name: (6R,7R)-7-[2-(2-Amino-4-thiazolyl) glyoxylamido]-8-oxo-3-vinyl-5-thia-1-azabicyclo [4.2.0] oct-2-ene-2-carboxylic acid, 72-(Z)- [O-(carboxy methyl) oxime] trihydrate
Chemical Formula: C16H15N5O7S2.3H2O
Molecular Weight: 507.50
Structure:
Ofloxacin
Chemical Name: (±)-9-fluoro-2,3-dihydro-3-methyl-10-(4-methyl-1- piperazinyl)-7-oxo-7H-pyrido[1,2,3-de]-1,4-benzoxazine6-carboxylic acid
Chemical Formula: C18H20FN3O4
Molecular Weight: 361.4
Structure:

8.0 Pharmaceutical particulars
8.1 Incompatibilities
None
8.2 Shelf-life
Refer on the pack
8.3 Packaging information
A blister strip of 10 tablets.
8.4 Storage and handing instructions
Store below 25°C. Protect from light
Keep out of reach of children.
9.0 Patient Counselling Information
- Counsel patients that antibacterial drugs should only be used to treat bacterial infections. They do not treat viral infections (e.g., the common cold). When C Tax-OF is prescribed to treat a bacterial infection, patients should be told that although it is common to feel better early in the course of therapy, the medication should be taken exactly as directed. Skipping doses or not completing the full course of therapy may: (1) decrease the effectiveness of the immediate treatment and (2) increase the likelihood that bacteria will develop resistance and will not be treatable by C Tax- OF or other antibacterial drugs in the future.
- Advise patients to contact their healthcare provider if they experience pain, swelling, or inflammation of a tendon, or weakness or inability to use one of their joints; rest and refrain from exercise; and discontinue C Tax-OF treatment. The risk of severe tendon disorders with fluoroquinolones is higher in older patients usually over 60 years of age, in patients taking corticosteroid drugs, and in patients with kidney, heart or lung transplants;
- Advise patients that diarrhea is a common problem caused by antibacterial drugs which usually ends when the antibacterial drug is discontinued. Sometimes after starting treatment with antibacterial drugs, patients can develop watery and bloody stools (with or without stomach cramps and fever) even as late as two or more months after having taken the last dose of the antibacterial drug. If this occurs, patients should contact their physician as soon as possible.
- Advise patients that peripheral neuropathies have been associated with ofloxacin use. If symptoms of peripheral neuropathy including pain, burning, tingling, numbness, and/or weakness develop, they should discontinue treatment and contact their physicians
- photosensitivity/phototoxicity has been reported in patients receiving quinolone antibiotics. Patients should minimize or avoid exposure to natural or artificial sunlight (tanning beds or UVA/B treatment) while taking quinolones. If patients need to be outdoors while using quinolones, they should wear loose-fitting clothes that protect skin from sun exposure and discuss other sun protection measures with their physician. If a sunburn-like reaction or skin eruption occurs, patients should contact their physician.
- if they are diabetic and are being treated with insulin or an oral hypoglycemic drug, to discontinue ofloxacin immediately if a hypoglycemic reaction occurs and consult a physician
- convulsions have been reported in patients taking quinolones, including ofloxacin, and to notify their physician before taking this drug if there is a history of this condition
- if they are diabetic and are being treated with insulin or an oral hypoglycemic drug, to discontinue C Tax-OF immediately if a hypoglycemic reaction occurs and consult a physician
- Patients are advised to inform their physician of any personal or family history of QTc prolongation or proarrhythmic conditions such as hypokalemia, bradycardia, or recent myocardial ischemia; if they are taking any class IA (quinidine, procainamide), or class III (amiodarone, sotalol) antiarrhythmic agents. Patients should notify their physicians f they have any symptoms of prolongation of the QTc interval including prolonged heart palpitations or a loss of consciousness.
- Tell the patients if they get any side effects, talk to the doctor. This includes any possible side effects not listed in this leaflet. Advice patients if they have any further questions, ask the doctor or pharmacist.
12.0 Date of revision of text
05-07-2024
About Leaflet
Read all of this leaflet carefully before your child starts taking this medicine because it contains important information for you.
- Keep this leaflet. You may need to read it again.
- If you have any further questions, ask your doctor or pharmacist.
- This medicine has been prescribed for your child. Do not pass it on to others. It may harm them, even if their signs of illness are the same as your child’s.
- If your child gets any side effects, talk to your doctor or pharmacist. This includes any possible side effects not listed in this leaflet.
What is in this leaflet?
- What C Tax-OF tablet is and what it is used for?
- What you need to know before you take C Tax-OF tablet?
- How to take C Tax-OF tablet?
- Possible side effects
- How to store C Tax-OF tablet?
- Contents of the pack and other information
1. What C Tax-OF tablet is and what it is used for?
C Tax-OF tablet is a combination of two medicines: Cefixime and Ofloxacin. Cefixime belongs to a group of antibiotics called “cephalosporin”. Ofloxacin belongs to a group of medicines called “quinolone antibiotics”.
Cefixime kills bacteria by preventing them from building their cell walls, while ofloxacin kills bacteria by stopping them from making and repairing their DNA. Without a cell wall or functional DNA, the bacteria cannot survive.
C Tax-OF tablets is specifically used for typhoid fever and urinary tract infections in adults.
2. What you need to know before you take C Tax-OF Tablet?
Do not take C Tax-OF Tablet if you:
- Are allergic to cefixime, ofloxacin, cephalosporins, or quinolones. Signs of an allergic reaction include: a rash, swallowing or breathing problems, swelling of your lips, face, throat or tongue.
- Have a history of tendinitis (inflammation or swelling of tendons) or tendon rupture related to fluoroquinolone use.
- Have epilepsy or a history of seizures/fits.
- Are pregnant, think you may be pregnant or are planning to have a baby
- Are breastfeeding.
- If you are under the age of 18 years, or are still growing
- If you suffer from or there is a family history of glucose-6-phosphate dehydrogenase deficiency (an inherited disorder that affects the red blood cells)
Do not take this medicine if any of the above apply to you. If you are not sure, talk to your doctor or pharmacist before taking C Tax-OF tablets.
Warnings and Precautions:
Talk to your doctor or pharmacist before taking C Tax-OF tablets if any of the following apply:
- if you have been diagnosed with an enlargement or "bulge" of a large blood vessel (aortic aneurysm or large vessel peripheral aneurysm)
- if you have a family history of aortic aneurysm or aortic dissection or congenital heart valve disease, or other risk factors or predisposing conditions (e.g. connective tissue disorders such as Marfan syndrome or Ehlers- Danlos syndrome, Turner syndrome, Sjögren’s syndrome (an inflammatory autoimmune disease) or vascular disorders such as Takayasu arteritis, giant cell arteritis, Behcet’s disease, high blood pressure, or known atherosclerosis, rheumatoid arthritis (a disease of the joints) or endocarditis (an infection of the heart))
- you have or have ever had a history of mental illness.
- you have problems with your liver or kidneys.
- you have heart disease or problems with your heartbeat
- you were born with or have family history of prolonged QT interval (seen on ECG, electrical recording of the heart).
- have salt imbalance in the blood (especially low level of potassium or magnesium in the blood)
- have a weak heart (heart failure)
- have a history of heart attack (myocardial infarction)
- you have an illness of the nervous system called ‘myasthenia gravis’ (muscle weakness)
- you have diabetes or blood sugar problems, as this medication can cause low blood sugar (hypoglycemia)
- Avoid strong sunlight or artificial UV rays during and for 48 hours after treatment.
During treatment
When taking this medicine
- If your eyesight becomes impaired or if your eyes seem to be otherwise affected, consult an eye specialist immediately
- If you feel sudden, severe pain in your abdomen, chest or back, which can be symptoms of aortic aneurysm and dissection, go immediately to an emergency room. Your risk may be increased if you are being treated with systemic corticosteroids
- If you start experiencing a rapid onset of shortness of breath, especially when you lie down flat in your bed, or you notice swelling of your ankles, feet or abdomen, or a new onset of heart palpitations (sensation of rapid or irregular heartbeat), you should inform a doctor immediately
- Pain and swelling in the joints and inflammation or rupture of tendons may occur rarely. Your risk is increased if you are elderly (above 60 years of age), have received an organ transplant, have kidney problems or if you are being treated with corticosteroids. Inflammation and ruptures of tendons may occur within the first 48 hours of treatment and even up to several months after stopping of C Tax-OF therapy. At the first sign of pain or inflammation of a tendon (for example in your ankle, wrist, elbow, shoulder or knee), stop taking C Tax-OF, contact your doctor and rest the painful area. Avoid any unnecessary exercise as this might increase the risk of a tendon rupture.
- You may rarely experience symptoms of nerve damage (neuropathy) such as pain, burning, tingling, numbness and/or weakness especially in the feet and legs or hands and arms. If this happens, stop taking C Tax-OF and inform your doctor immediately in order to prevent the development of potentially irreversible condition.
If you are not sure if any of the above apply to you, talk to your doctor or pharmacist before taking C Tax-OF.
Other medicines and C Tax-OF Tablet:
Tell your doctor or pharmacist if you are taking, have recently taken or might take any other medicines.
- medicines or dietary supplements that contain iron (for anaemia) or zinc.
- sucralfate used for stomach ulcers.
- antacids used for indigestion that contain magnesium or aluminium.
- corticosteroids, used for treatment of inflammation and swelling or over-active immune system. These may increase the risk of you developing a tendon rupture
- painkillers called non-steroidal anti-inflammatory drugs (NSAIDs) e.g. ibuprofen or diclofenac, or theophylline, used to treat asthma or chronic obstructive pulmonary disease as these could make you more prone to fits if taken with C Tax-OF tablet.
- glibenclamide, a medicine to control your blood sugar, as the amount of these medicines in the blood may increase and have a greater effect.
- drugs that may affect your kidney function e.g. cimetidine (used for stomach ulcers or indigestion), probenecid (used for gout) and methotrexate (used for rheumatism) as they can increase the level of ofloxacin in the blood.
- medicines to thin your blood, e.g. warfarin.
- water tablets (diuretics) such as furosemide
This medicine should not be taken within two hours of taking iron or zinc tablets, antacids, or sucralfate, as these medicines can stop C Tax-OF tablet from working properly.
If you are due to have urine tests for porphyrin (a pigment in the blood), or for opiates (strong painkillers), tell your doctor or nurse you are taking this medicine.
Pregnancy and breast-feeding
Do not take C Tax-OF tablet if you are pregnant or breast-feeding, think you may be pregnant or are planning to have a baby. If you become pregnant while taking C Tax-OF tablet, stop taking the tablets and contact your doctor immediately.
Driving and using machines
Taking C Tax-OF tablet may make you feel sleepy, dizzy or could affect your eyesight. Do not drive or use machines until you know how this medicine affects you. Drinking alcohol may make these symptoms worse.
3. How to take C Tax-OF Tablet?
Always take this medicine exactly as your doctor or pharmacist has told you. Check with your doctor or pharmacist if you are not sure.
- For oral use. You should swallow these tablets whole with water. Do not chew them.
- The tablets can be taken with or without food and can be divided into equal doses.
- When taking C Tax-OF, avoid strong sunlight and do not use sun lamps or solaria as your skin may be more sensitive to light.
- If you are taking iron tablets (for anaemia), antacids (for indigestion or heartburn) or sucralfate (for stomach ulcers), it is important not to take these two hours before or after taking C Tax-OF. If you feel the effect of your medicine is too weak or strong, do not change the dose yourself, but ask your doctor.
- When taking C Tax-OF, if your eyesight becomes impaired or if your eyes seem to be otherwise affected, consult an eye specialist immediately
Dosage in Adults:
Take 1 tablet twice daily, as directed by your doctor.
Use in children and adolescents:
Children or adolescents under 18 years of age should not take these tablets.
If you take more C Tax-OF tablet:
If you take more tablets than you should you may become confused and dizzy or lose consciousness, you may have a seizure or fit, and you may feel sick. Contact your doctor or nearest hospital casualty department immediately. Take the container and any remaining tablets with you.
If you forget to take C Tax-OF tablet:
If you forget to take a dose take it as soon as you remember unless it is nearly time for your next dose. Do not take a double dose to make up for a forgotten tablet
If you stop taking C Tax-OF tablet:
Your doctor will tell you how long you need to take your tablets for. Do not suddenly stop taking this medicine without talking to your doctor first. If you stop, your infection may get worse again. If you feel the effect of your medicine is too weak or strong, do not change the dose yourself, but ask your doctor.
If you have any further questions on the use of this medicine, ask your doctor or pharmacist.
4. Possible side-effects
Like all medicines, this medicine can cause side effects, although not everybody gets them. Stop taking C Tax-OF, tell your doctor or go to your nearest hospital casualty department straight away if you have any of the following serious side effects because you may need medical attention:
With Ofloxacin:
Uncommon (may affect up to 1 in 100 people)
resistance of infection causing organisms to this treatment, (you may fail to respond to treatment)
Rare (may affect up to 1 in 1,000 people):
- you have an allergic reaction. Such reactions may appear in the form of anaphylaxis (a severe form of allergic reaction) with symptoms such as: - severe skin rash - swelling of the face, lips, mouth, tongue or throat (angioedema) - anaphylactic shock (sudden wheezing, swelling of your lips, tongue and throat or body, rash, fainting or difficulties in swallowing)
- inflammation of the bowel, which may cause severe watery diarrhoea, which may have blood in it, possibly with stomach cramps and a high temperature
- swelling of the tendons with the following symptoms; pain, tenderness, sometimes restricted movement (tendonitis). This can lead to tendon rupture, especially of the large tendon at the back of the ankle (Achilles tendon). The risk of this occurring is increased if you are also taking corticosteroids e.g. prednisolone
- numbness or tingling in the hands and feet or being very sensitive to touch, numbness or weakness of the arms and legs
- blurred, double or altered colour vision. If your eyesight becomes impaired or if your eyes seem to be otherwise affected, consult an eye specialist immediately.
Very rare (may affect up to 1 in 10,000 people):
- a condition in which the amount of oxygen-carrying pigment (haemoglobin) in the blood is below normal or an illness resulting from the destruction of red blood cells with the following symptoms; feeling tired, faint, dizzy, being short of breath when exercising and having pale skin. These may be signs of anaemia or haemolytic anaemia.
- other blood disorders when the numbers of different types of cells in the blood may fall, which may cause fever, chills, sore throat, ulcers in the mouth and throat (leucopenia, agranulocytosis)
- fits (seizures)
- skin rash, which may blister, and looks like small targets (central dark spots surrounded by a paler area, with dark ring around the edge) (erythema multiforme)
- a widespread rash with blisters and skin peeling on much of the body surface (toxic epidermal necrolysis).
- narrowing, blockage or leakage of blood vessels, in exceptional cases leading to severe skin reactions and death of areas of the skin
- severe kidney problems, which may result in your kidneys stopping working. Signs may include a rash, high temperature, general aches and pains, or blood in the urine
- hearing problems or hearing loss
- liver problems, such as inflammation of the liver (hepatitis) or blockage in the bile duct, that may cause your eyes or skin to go yellow (jaundice) or you may notice the following symptoms; nausea, vomiting, loss of appetite, feeling generally unwell, fever, itching, light coloured bowel motions, dark coloured urine
With Cefixime:
- liver problems, such as inflammation of the liver (hepatitis) or blockage in the bile duct, that may cause your eyes or skin to go yellow (jaundice) or you may notice the following symptoms; nausea, vomiting, loss of appetite, feeling generally unwell, fever, itching, light coloured bowel motions, dark coloured urine
- DRESS symptoms may include flu-like symptoms and a widespread rash with a high body temperature and enlarged lymph nodes. Abnormal blood test results may include increased levels of liver enzymes and an increase in a type of white blood cell (eosinophilia) and enlarged lymph nodes.
- AGEP symptoms may include a red, scaly, widespread rash with bumps under the skin (including your skin folds, chest, abdomen (including stomach), back and arms) and blisters accompanied by fever.
- Erythema multiforme symptoms include skin rash or skin lesions with a pink/red ring and a pale centre which may be itchy, scaly or filled with fluid. The rash may appear especially on the palms or soles of your feet.
- You get infections more easily than usual. This could be because of a blood disorder. This normally gets better after stopping the medicine.
- You bruise or bleed more easily than normal. This could be because of a blood disorder. This normally gets better after stopping the medicine.
- If your child gets nose bleeds, bleeding gums, chills, tiredness, pale skin (often with a yellow tinge), shortness of breath. This may be due to haemolytic anaemia
- A brain condition with symptoms including fits (convulsions), feeling confused, feeling less alert or aware of things than usual, unusual muscle movements or stiffness. This may be something called encephalopathy. This side effect is more likely if you have taken an overdose or you already have a problem with your kidneys.
Reporting of side effects
If you get any side effects, talk to your doctor, pharmacist or nurse. This includes any possible side effects not listed in this leaflet. You can also report side effects directly:
Website: www.zuventus.com and click the tab “Safety Reporting” located on the top end of the home page.
Website link: https://www.zuventus.com/drug-safety-reporting
By reporting side effects, you can help provide more information on the safety of this medicine. You can also report the side effect with the help of your treating physician.
5. How to store C Tax-OF tablet?
Keep this medicine out of the sight and reach of children. Do not take this medicine after the expiry date shown on the pack.
The expiry date refers to the last day of that month.
Store below 25°C. Protect from light & moisture
6. Contents of the pack and other information
What C Tax-OF contains
Each film coated tablet contains:
Cefixime (as Trihydrate) IP equivalent to Anhydrous Cefixime 200 mg
Ofloxacin IP 200 mg
Excipients q.s.
Colours: Lake of Quinoline Yellow & Titanium Dioxide IP
Packaging information
A blister strip of 10 tablets.
Marketing Authorisation Holder
Zuventus Heathcare Ltd. Zuventus House,
Plot Y2, CTS No: 358/A2,
Near Nahur Railway Station,
Nahur (West), Mumbai 400 078.
This leaflet was last revised in July 2024
For More Information About This Product
Brophyle SR Tablets
1.0 Generic name
Acebrophylline Prolonged release Tablets
2.0 Qualitative and quantitative composition
Each uncoated prolonged-release tablet contains:
Acebrophylline……………………………………. 200 mg
Excipients q.s.
3.0 Dosage form and strength
Tablet 200 mg
4.0 Clinical particulars
4.1 Therapeutic indication
For the treatment of adult patients with chronic obstructive pulmonary disease (COPD) and bronchial asthma.
4.2 Posology and method of administration
Adults
Acebrophylline is administered at a recommended dose of 1 tablet once daily.
4.3 Contraindications
Hypersensitivity to xanthine derivatives like theophylline or to ambroxol.
4.4 Special warnings and precautions for use
Acebrophylline should be administered with caution in patients with hypertension, heart diseases, peptic ulcers and severe hypoxemia.
4.5 Drugs interactions
Theophylline should not be administered concurrently with other xanthine preparations and caution is required due to the interaction between theophylline and ephedrine or other sympathomimetic bronchodilators. The concomitant administration of reserpine may result in tachycardia.
4.6 Use in special populations
Pregnancy & Lactation
Although there are no clinical studies in pregnant or lactating women, Acebrophylline should be avoided in these women, unless the benefits outweigh the risks.
4.7 Effects on ability to drive and use machines
Brophyle SR Tablet does not usually affect the ability to drive.
4.8 Undesirable effects
Commonly reported adverse effects with Acebrophylline include abdominal discomfort, stomach/abdominal distension, vomiting, abdominal pain, diarrhea, constipation, heart burn, loss of appetite, esophageal bleeding, rashes, urticaria, itching, drowsiness, difficulty in breathing, leukocytosis and nasal inflammation. If chills and fever occur the drug should be immediately discontinued.
Rarely occurring adverse events include headache, occasional numbness including numbness in arm, insomnia, tachycardia, fatigue, hypertension, albuminuria, glycosuria, hypotension and occasionally hyperglycemia.
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via email to: medico@zuventus.com
Website: https://www.zuventus.com/drug-safety-reporting
By reporting side effects, you can help provide more information on the safety of this medicine.
4.9 Overdose
In the event of overdose, the stomach may be emptied by gastric lavage within 2 hrs of overdose. Elimination may also be enhanced by repeated oral doses of activated charcoal. Treatment is symptomatic and supportive.
5.0 Pharmacological properties
5.1 Mechanism of Action / Pharmacodynamic Properties
Acebrophylline is an airway mucus regulator with anti-inflammatory actions. It has a multimodal mechanism of action involving effects on the pulmonary surfactant, bronchial secretions, phospholipase A and Phosphodiesterases. Theophylline-7-acetate, as with other xanthine derivatives, has a bronchodilator effect due to inhibition of the intracellular phosphodiesterases, followed by an increase of cyclic adenosine monophosphate levels, which promote the relaxation of bronchial muscles. Acebrophylline produces bronchodilation by specifically inhibiting phosphodiesterase III and IV.
Acebrophylline inhibits phospholipase A, and phosphatidylcholine leading to lesser production of the powerful pro-inflammatory substances like leukotrienes and tumour necrosis factor. By inhibiting the synthesis and release of these inflammatory mediators, Acebrophylline reduces inflammation, a key factor in airway obstruction, especially in chronic forms.
Acebrophylline increases the synthesis and secretion of pulmonary surfactants by acting on two levels of surfactant synthesis: the first involving ambroxol’s established action on phosphocholine-cytidyl-transferase and the second probably because of theophylline-7 acetic acid’s action on choline-kinase.
Ambroxol modifies the mucous gel phase of secretions by decreasing the viscosity and increasing the serous gel phase. It increases the mucociliary clearance by stimulating cilia motility. Thus, it has mucoregulatory, mucosecretory as well as mucokinetic actions, thereby normalizing the quantity & quality of pulmonary secretions.
5.2 Pharmacokinetic properties
On administration of 200 mg SR oral Acebrophylline, the two components of the molecule – ambroxol and theophylline-7-acetate are released in the stomach and absorbed in the intestines, reaching optimal concentrations of ambroxol and very low levels of theophylline- 7- acetic acid.
Thus it appears that the latter is either poorly absorbed or metabolized very fast and is eliminated in a fairly short time. Its low blood levels mean it is not likely to cause the untoward effects seen after theophylline, whose therapeutic window corresponds to much higher plasma concentrations (10-20 mcg/mL). Acebrophylline reaches its peak in serum (mean Cmax 136.458 +/- 7.079 ng/mL) at 1.708 +/- 0.550 hrs.
The elimination half-life of Acebrophylline is about 6.632 +/- 0.439 hrs. The drug is metabolized in the liver and eliminated renally.
6.0 Nonclinical properties
6.1 Animal Toxicology or Pharmacology
No known animal toxicology data
7.0 Description
Acebrophylline (Ambroxol theophylline-7-acetate) is the salt obtained by reaction of equimolar amounts of ambroxol, a drug showing mucolytic and expectorant properties, and theophylline-7-acetic acid, a xanthine derivative with specific bronchodilator activity.
Acebrophylline is obtained by targeted salification of the ambroxol base [trans-4(2-amino-3, 5 dibromobenzylamino)cyclohexanol] and theophylline 7 acetic acid. The carboxyl group of theophylline-7-acetic acid is salified with ambroxol’s amine group in a stoichiometric ratio (38.7% acid and 61.3% base) that ensures, after absorption, high plasma levels of ambroxol with low levels of the xanthine derivative which are nevertheless high enough to ensure a carrier effect for ambroxol. This means that one hour after administration lung levels of ambroxol are 45% higher than in subjects treated with ambroxol alone.
Its molecular formula is C22H28Br2N6O5 and its molecular weight is 616.3.
8.0 Pharmaceutical particulars
8.1 Incompatibilities
Not applicable
8.2 Shelf-life
Refer on pack
8.3 Storage and handing instructions
Store below 30°C. Protect from light & moisture.
Keep out of reach of children.
9.0 Patient counselling information
- You have been prescribed Brophyle SR Tablet for prevention and treatment of asthma and chronic obstructive pulmonary disease (COPD).
- It should be taken at the same time each day, preferably in the evening after food.
- It does not work right away and should not be used to relieve sudden breathing problems. Always keep a fast-acting (rescue) inhaler with you.
- Your doctor may take regular blood test to monitor potassium level and the level of this medicine in your body.
- Notify your doctor if you have ever been diagnosed with kidney, liver or heart disease, or if you have a smoking history. Your dose may need to be adjusted.
- Do not discontinue use without consulting your doctor, even if you feel better.
12.0 Date of revision
16.09.2022
About leaflet
Please read this leaflet carefully before you start using this medicine because it contains important information for you.
- Keep this leaflet. You may need to read it again.
- If you have any further questions, ask your doctor or pharmacist.
- This medicine has been prescribed for you. Do not pass it on to others. It may harm them, even if their signs of illness are the same as yours.
- If you get any side effects, talk to your doctor or pharmacist. This includes any possible side effects not listed in this leaflet.
What is in this leaflet
1. What Brophyle SR is and what it is used for
2. What you need to know before you use Brophyle SR
3. How to use Brophyle SR
4. Possible side effects
5. How to store Brophyle SR
6. Contents of the pack and other information
1. What Brophyle SR is and what it is used for
Brophyle SR contains the active substance acebrophylline, which is used to treat adult patients with chronic obstructive pulmonary disease (COPD) and bronchial asthma. It helps to reduce inflammation and relax the muscles in the airways, making it easier to breathe.
2. What you need to know before you use Brophyle SR
Do not take Brophyle SR if you:
- Are allergic to acebrophylline, theophylline, ambroxol, or any of the other ingredients of this medicine.
- Have a history of hypersensitivity to xanthine derivatives.
Warnings and precautions: Talk to your doctor or pharmacist before taking Brophyle SR if you:
- Have hypertension, heart diseases, peptic ulcers, or severe hypoxemia.
- Are pregnant or breastfeeding. This medicine should be avoided unless the benefits outweigh the risks.
Other medicines and Brophyle SR: Tell your doctor or pharmacist if you are taking, have recently taken, or might take any other medicines, especially:
- Other xanthine preparations
- Sympathomimetic bronchodilators (e.g., ephedrine)
- Reserpine
Important Precautions
- You have been prescribed Brophyle SR Tablet for prevention and treatment of asthma and chronic obstructive pulmonary disease (COPD).
- It should be taken at the same time each day, preferably in the evening after food. It does not work right away and should not be used to relieve sudden breathing problems. Always keep a fast-acting (rescue) inhaler with you.
- Your doctor may take regular blood test to monitor potassium level and the level of this medicine in your body.
- Notify your doctor if you have ever been diagnosed with kidney, liver or heart disease, or if you have a smoking history. Your dose may need to be adjusted.
- Do not discontinue use without consulting your doctor, even if you feel better.
3. How to take Brophyle SR
Always take this medicine exactly as your doctor or pharmacist has told you. Check with your doctor or pharmacist if you are not sure.
Adults:
- The recommended dose is one tablet once daily, preferably in the evening after food.
If you take more Brophyle SR than you should
Contact your doctor or go to the nearest hospital emergency department immediately. Symptoms of overdose may include nausea, vomiting, abdominal pain, and tachycardia.
If you forget to use Brophyle SR
If you forget to take at the right time, use it as soon as you remember, then carry on as before. Do not take a double dose to make up for a forgotten dose.
If you stop using Brophyle SR
Do not stop your treatment even if you feel better unless told to do so by your doctor.
Do not use in children.
If you have any further questions on the use of this medicine, ask your doctor, pharmacist or nurse.
4. Possible side effects
Like all medicines, this medicine can cause side effects, although not everybody gets them.
Common side effects:
- Abdominal discomfort, stomach distension, vomiting, abdominal pain, diarrhea, constipation, heartburn, loss of appetite, esophageal bleeding, rashes, urticaria, itching, drowsiness, difficulty in breathing, leukocytosis, nasal inflammation.
Rare side effects:
- Headache, numbness, insomnia, tachycardia, fatigue, hypertension, albuminuria, glycosuria, hypotension, hyperglycemia.
Reporting of side effects
If you get any side effects, talk to your doctor, pharmacist or nurse. This includes any possible side effects not listed in this leaflet. You can also report side effects directly: Website: www.zuventus.com and click the tab “Drug Safety Reporting” located on the top end of the home page. Website link: https://www.zuventus.com/drug-safety-reporting. By reporting side effects, you can help provide more information on the safety of this medicine. You can also report the side effect with the help of your treating physician.
5. How to store Brophyle SR
- Keep this medicine out of the sight and reach of children.
- Store below 30°C. Protect from light and moisture.
- Do not use this medicine after the expiry date which is stated on the pack.
- Do not throw away any medicines via wastewater or household waste. Ask your pharmacist how to throw away medicines you no longer use. These measures will help protect the environment.
6. Contents of the pack and other information
What Brophyle SR contains
The active substance is acebrophylline
Each tablet contains 200 mg of acebrophylline
For More Information About This Product
Bevon Capsules
1.0 Generic name
Multivitamin, Multimineral & Antioxidants Capsules
2.0 Qualitative and quantitative composition
Each soft gelatin capsule contains:
Pyridoxine Hydrochloride IP 1.5 mg
Niacinamide IP 15 mg
Cyanocobalamin IP 0.5 mcg
Folic Acid IP 300 mcg
Choline Bitartrate USP 10 mg
Biotin IP 30 mcg
Betacarotene (30% Dispersion) USP 5 mg
Nickel Sulphate equivalent to Elemental Nickel 15 mcg
Zinc Sulphate Monohydrate IP equivalent to Elemental Zinc 7.5 mg
Sodium Selenite Pentahydrate BP equivalent to Elemental Selenium 30 mcg
Copper Sulphate Pentahydrate BP equivalent to Elemental Copper 2.5 mg
Chromium Picolinate IP equivalent to Elemental Chromium 65 mcg
Manganese Sulphate USP equivalent to Elemental Manganese 1.4 mg
Sodium Molybdate Dihydrate BP equivalent to Elemental Molybdenum 25 mcg
Benfotiamine 2 mg
Sodium Borate BP equivalent to Elemental Boron 150 mcg
Dibasic Calcium Phosphate IP equivalent to Elemental Phosphorous 125 mg
Lycopene Preparations (10%) USP 5 mg
Excipients q.s.
In wheat germ oil virgin & flaxseed oil base.
Approved colours used in the capsule shell.
Appropriate overages of Vitamins added.
3.0 Dosage form and strength
Soft gelatin capsule.
4.0 Clinical particulars
4.1 Therapeutic Indications
For Vitamins and Mineral deficiency states in adult patients
4.2 Posology and method of administration
Adults and the Elderly:
One capsule daily. Preferably taken one hour after meals. Do not exceed the stated dose.
The capsule should be swallowed whole with water.
Children under 12 years of age:
Bevon Capsules are not recommended for this age group.
4.3 Contraindications
Hypersensitivity to the active substance or to any of the excipients listed in the formulation.
4.4 Special warnings and precautions for use
- Whilst taking Bevon Capsules both protein and energy are also required to provide complete nutrition in the daily diet. No other vitamins, minerals or supplements with or without vitamin A should be taken with this preparation except under medical supervision.
- Do not take Bevon Capsules on an empty stomach. Do not exceed the stated dose. Keep out of the reach of children. If symptoms persist, consult your doctor.
- Evidence from Randomised Control Trials suggests that high doses (20-30 mg/day) β-carotene intake may increase the risk of lung cancer in current smokers and those previously exposed to asbestos. This high-risk population should consider the potential risks and benefits of Bevon Capsules, which contain 5 mg of β-carotene per recommended daily dose, before use
4.5 Drug Interactions
Folic acid can reduce the plasma concentration of phenytoin. Zinc Sulphate reduce the absorption of tetracyclines.
4.6 Use in Special Populations
Pregnancy and Breastfeeding Bevon Capsules may be administered during pregnancy and lactation at the recommendation of the Physician.
4.7 Effects on ability to drive and use machines
None anticipated.
4.8 Undesirable effects
Immune system disorders: Hypersensitivity reaction (such as rash)
Gastrointestinal disorders: Gastrointestinal disturbances (such as nausea, vomiting and abdominal pain).
Reporting of suspected adverse reactions
- Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via email to: medico@zuventus.com
- Website: https://www.zuventus.com/drug-safety-reporting
By reporting side effects, you can help provide more information on the safety of this medicine.
4.9 Overdose
No cases of overdosage due to Bevon therapy have been reported. In case of accidental overdose, discontinue use and seek professional assistance immediately. Any symptoms which may be observed due to the ingestion of large quantities of capsules will be due to the fat soluble vitamin content. Gastric lavage may be necessary to remove drug already released into the stomach. Signs and symptoms such as gastrointestinal disorders like diarrhoea may be associated with an overdose of Bevon.
5.0 Pharmacological properties
5.1 Pharmacodynamic properties / Mechanism of action
Beta Carotene
β-carotene is the most prominent and efficient member of the group of carotenoids (natural colorants that occur in the human diet). Carotenoids are red, orange, or yellow, fat-soluble compounds. Alpha, beta, and gamma carotene are considered provitamins because they can be converted to active vitamin A. Beta-carotene is converted to retinol, which is essential for vision and growth. ROS-induced oxidative stress is suggested as being basic to several human diseases. β-carotene has a unique type of antioxidant activity. Beta carotene traps free radicals and studies suggest that it may also reduce tumor development. Studies have shown that vitamin A is essential to the normal growth of epithelial tissues.
Pyridoxine Hydrochloride
The active coenzyme form of vitamin B6 (Pyridoxine) is pyridoxal 5 ’-phosphate. Approximately 80% of the body's total vitamin B6 is present as pyridoxal phosphate in muscle. Pyridoxal phosphate is a coenzyme for many enzymes involved in amino acid metabolism. It is also the co-factor for glycogen phosphorylase, where the phosphate group is catalytically important. Vitamin B6 helps the body to make several neurotransmitters. It is needed for normal brain development and function, and helps the body to make the hormones serotonin and norepinephrine, which influence mood, and melatonin, which helps to regulate the body clock. Along with vitamins B12 and B9 (folicacid), B6 helps to control levels of homocysteine in the blood. In addition, vitamin B6 is important in steroid hormone action where it removes the hormone-receptor complex from DNA binding, terminating the action of the hormones. In vitamin B6 deficiency, this results in increased sensitivity to the actions of low concentrations of estrogens, androgens, cortisol and vitamin D.
Folic Acid
Folate is a water-soluble B-vitamin and enzymatic cofactor that is necessary for the synthesis of purine and thymidine nucleotides as well as for synthesis of methionine from homocysteine. Tetrahydrofolate (TH4-folate) is the biologically active form of folic acid. The main role of folic acid in biochemistry is the single-carbon transfer reaction (e.g. transfer of a methyl, methylene, or formyl group). Folic acid is involved in the transformation of certain amino acids as well as in the synthesis of purines and dTMP (2'-deoxythymidine-5'-phosphate) needed for the synthesis of nucleic acid (DNA), required by all rapidly growing cells. In humans, folate deficiency results in serious pathologies, the most important of which are neural tube defects, megablastic anemia, acceleration of the arteriosclerotic process, changes in the central nervous system, and the development of certain types of cancer.
Cyanocobalamin
Vitamin B12 is found only in foods of animal origin. Vitamin B12 is essential for cellular DNA synthesis and hence contributes to functions of various tissues of the body, formation of myelin sheath, more so the rapidly dividing and proliferating cellular systems such as blood and gastric epithelium. The absorbed inert form of cyanocobalamin is converted into two important active forms. One is methylcobalamin-involved in maturation of red blood corpuscles. The second active form is adenosylcobalamin involved in healthy myelination and neuronal integrity. Methylcobalamin deficiency leads to folate trap resulting in megaloblastic anemia. Deficiency of adenosylcobalamin leads to accumulation of large amount of methylmalonyl-CoA resulting in synthesis and incorporation of nonphysiological fatty acids into neuronal lipids, causing, demyelination, axonal degeneration and neuronal death leading to neurological complications.
Zinc Sulphate
Zinc is an essential trace mineral necessary for the proper function of about 300 different enzymes. Therefore, zinc plays a role in virtually all biochemical pathways and physiological processes in the body. Thirty percent of the body's zinc is stored in the bones and 60% in muscles. The other 10% is found in virtually all body tissues. Zinc is important for wound healing, immune system support and to increase fertility (sperm production). It also assists digestion, energy production, growth, cellular repair, collagen synthesis, bone strength, cognitive function, and carbohydrate metabolism (glucose utilization and insulin production). Zinc not only modulates cell-mediated immunity but is also an antioxidant and anti-inflammatory agent. Mild zinc deficiencies are currently thought to cause chronic metabolic derangement leading to or exacerbating immune deficiency, gastrointestinal problems, endocrine disorders, neurologic dysfunction, cancer, accelerated aging, degenerative disease, and more.
Niacinamide
Niacin was discovered as a nutrient during studies of pellagra. It is not strictly a vitamin since it can be synthesized in the body from the essential amino acid tryptophan. Two compounds, nicotinic acid and nicotinamide, have the biologic activity of niacin; its metabolic function is as the nicotinamide ring of the coenzymes NAD and NADP in oxidation-reduction reactions. Nicotinamide has important role in DNA repair mechanism.
Biotin
Biotin (Vitamin B7 or H) is a water soluble B vitamin that is essential for bodily health. It helps the body to process fat and sugars, and it helps form a critical process in fat production in the body. Biotin is involved in a number of carboxylase reactions. Biotin is often recommended as a dietary supplement for healthy skin, hair and nails. Biotin deficiency is characterized by development of a fine scaly dermatitis, hair loss, conjunctivitis, ataxia and delayed development.
Sodium Molybdate Dihydrate
Molybdenum belongs to a group of essential microelements. Molybdenum-containing enzymes catalyze basic metabolic reactions in the nitrogen, sulfur, and carbon cycles and are important for variety of metabolic pathways.
Copper Sulphate Pentahydrate
Copper is a trace element present in all tissues and is required for cellular respiration, peptide amidation, neurotransmitter biosynthesis, pigment formation, and connective tissue strength. Copper is a cofactor for numerous enzymes and plays an important role in central nervous system development. Copper is essential for brain development during foetal and post-natal growth, and maintenance of brain health throughout life (including effective anti-oxidative defence), efficient communication between nerve cells, maintenance of healthy skin and connective tissue, wound healing, structural integrity and function of heart and blood vessels, growth of new blood vessels, proper structure and function of circulating blood cells, formation of the cells of immune system, maintenance of a healthy and effective immune response and generation and storage of energy in the mitochondria.
Sodium Selenate
Selenium is incorporated into selenoproteins that have a wide range of pleiotropic effects, ranging from antioxidant, immune functions and anti-inflammatory effects to the production of active thyroid hormone. Low selenium status has been associated with increased risk of mortality, poor immune function, and cognitive decline. Selenium supplementation has antiviral effects, is essential for male and female reproduction, and reduces the risk of autoimmune thyroid disease. Prospective studies have generally shown some benefit of higher selenium status on the risk of various cancers.
Chromium Picolinate
Chromium is a critical cofactor in the action of insulin. Results from some trials have indicated that chromium supplementation increases muscle gain and fat loss associated with exercise and improves glucose metabolism and the serum lipid profile in patients with or without diabetes. Low chromium levels can increase blood sugar, triglycerides, cholesterol levels, and increase the risk for a number of conditions, such as diabetes and heart disease.
Manganese Sulphate
Manganese is an essential element for humans and is required for growth, development, and maintenance of health. Manganese is necessary for a variety of metabolic functions including those involved in skeletal system development, energy metabolism, activation of certain enzymes, nervous system function, immunological system function, and reproductive hormone function. It is an antioxidant that protects cells from damage due to free radicals. Manganese also plays an essential role in regulation of cellular energy, bone and connective tissue growth and blood clotting. In the brain, Manganese is an important cofactor for a variety of enzymes, including the antioxidant enzyme superoxide dismutase, as well as enzymes involved in neurotransmitter synthesis and metabolism.
Choline Bitartrate
Choline is a component of phosphatidylcholine, acetylcholine, lecithin, sphingomyelin, cell membranes, plasma lipoproteins and platelet activating factors. Lecithin and sphingomyelin participate in signal transduction, an essential process for cell growth, regulation and function.
Benfotiamine
Thiamine (Vitamin B1) is considered as an essential micronutrient for humans. Due to the low bioavailability of the hydrosoluble forms of thiamine, its liposoluble preparations (benfotiamine) are preferentially used. Benfotiamine, a lipid-soluble analogue of vitamin B1, is a potent antioxidant that is used as a food supplement. Once thiamine enters the cells, it is phosphorylated by thiamine pyrophosphokinase (TPPK), and converted into the coenzyme thiamine pyrophosphate (TPP), the active form of thiamine. TPP is a relevant cofactor for various enzymes fundamental for glucose metabolism. Recent evidences have shown that the administration of thiamine or lipid-soluble derivatives, such as benfotiamine, has positive effects in the diabetic patients. Numerous studies have shown that benfotiamine inhibits three major pathways that lead to the formation of toxic substances such as advanced glycation end products (AGEs).
Sodium Borate
Boron is a trace element which has an important influence on both calcium and magnesium metabolism. Boron is concentrated in the bone, spleen and thyroid indicating boron's functions in bone metabolism and suggesting its potential role in hormone metabolism. Boron is thought to be useful to increase muscle mass; increase muscle strength; maintain bone density; improve calcium absorption and decrease body fat. According to the USFDA, boron is a trace mineral that helps bones to develop and grow normally. Boron supplementation prevent atherosclerosis, improve brain function and cognitive functioning, reduce HDL cholesterol, affect thyroid hormone levels, alleviate harmful effects of vitamin D, magnesium, and potassium deficiency in postmenopausal bone loss, play a role in the prevention of osteoporosis and prevent calcium loss in postmenopausal women.
Nickel Sulphate
Nickel is a trace mineral that is required by body, but only in very small amount. Small amounts of nickel are found in DNA and RNA. Nickel plays a role in the circulation of some proteins and contributes to the production of hormones, lipids, and cell membranes. Nickel is also used to break down glucose for energy.
Dibasic Calcium Phosphate
Next to calcium, phosphorus is the most abundant mineral in the body. These 2 important nutrients work closely together to build strong bones and teeth. Phosphorus, an essential mineral, is naturally present in many foods and available as a dietary supplement. Phosphorus is a component of bones, teeth, DNA, and RNA. About 85% of phosphorus can be found in bones and teeth, but it is also present in cells and tissues throughout the body. The health benefits of phosphorous include healthy bone formation, provide strength to bones and teeth, improved digestion, regulated excretion, protein formation, hormonal balance, improved energy extraction, cellular repair, optimized chemical reactions and proper nutrient utilization. Phosphorus deficiency (hypophosphatemia) is rare in the United States and is almost never the result of low dietary intakes. The effects of hypophosphatemia can include anorexia, anemia, proximal muscle weakness, skeletal effects (bone pain, rickets, and osteomalacia), increased infection risk, paresthesias, ataxia, and confusion. In most cases, hypophosphatemia is caused by medical conditions, such as hyperparathyroidism, kidney tubule defects, and diabetic ketoacidosis.
Lycopene
Lycopene, a non-provitamin A carotenoid prominently present in red fruits such as tomatoes, exhibits several health benefits. Its potent antioxidant properties protect cells from oxidative stress, thereby reducing the risk of carcinogenesis, cardiovascular pathologies, diabetes and neurodegenerative ailments. Lycopene's potential in modulating lipid metabolism, particularly by attenuating low-density lipoprotein (LDL) cholesterol levels, thus confers cardioprotective effects. Lycopene's antioxidant and anti-inflammatory properties may aid in glycemic control and mitigating diabetic complications. It also exhibits a protective effect on ocular health by preventing age-related macular degeneration and cataractogenesis. Additionally, it is a nutraceutical that protects against a wide variety of heart, liver, bone, skin, nervous, and reproductive system diseases.
5.2 Pharmacokinetic properties
Beta Carotene
Except when liver function is impaired, Vitamin A is readily absorbed. β-carotene (as in Bevon Capsules) is Provitamin A and is the biological precursor to Vitamin A. It is converted to Vitamin A (Retinol) in the liver; retinol is emulsified by bile salts and phospholipids and absorbed in a micellar form. Part is conjugated with glucuronic acid in the kidney and part is metabolised in the liver and kidney, leaving 30 to 50% of the dose for storage in the liver. It is bound to a globulin in the blood. Metabolites of Vitamin A are excreted in the faeces and the urine.
Pyridoxine Hydrochloride
Pyridoxine is absorbed from the gastro-intestinal tract and converted to the active pyridoxal phosphate which is bound to plasma proteins. It is excreted in the urine as 4-pyridoxic acid.
Cyanocobalamin
Cyanocobalamin is absorbed from the gastro-intestinal tract and is extensively bound to specific plasma proteins. A study with labelled Vitamin B12 showed it was quickly taken up by the intestinal mucosa and held there for 2-3 hours. Peak concentrations in the blood and tissues did not occur until 8-12 hours after dosage with maximum concentrations in the liver within 24 hours. Cobalamins are stored in the liver, excreted in the bile and undergo enterohepatic recycling. Part of a dose is excreted in the urine, most of it in the first eight hours.
Dibasic Calcium Phosphate
The body contains from 600-800 g of phosphorus, over 80% of which is present in the bone as phosphate salts, mainly hydroxyapatite crystals. The phosphate in these crystals is available for exchange with phosphate ions in the extra-cellular fluids.
Folic Acid
Folic acid is absorbed mainly from the proximal part of the small intestine. Folate polyglutamates are considered to be deconjugated to monoglutamates during absorption. Folic acid rapidly appears in the blood where it is extensively bound to plasma proteins. Some folic acid is distributed in body tissues, some is excreted as folate in the urine and some is stored in the liver as folate.
Zinc Sulphate
Zinc is poorly absorbed from the gastro-intestinal tract. It is widely distributed throughout the body. It is excreted in the faeces with traces appearing in the urine.
Biotin
Following absorption, biotin is stored in the liver, kidney and pancreas.
Sodium Selenate
Although it has been established that selenium is essential to human life, very little information is available on its function and metabolism.
Chromium Picolinate
Most chromium compounds are soluble at the pH of the stomach, but less soluble hydroxides may form as pH is increased. The environment of the gastrointestinal tract and ligands provided by foods and supplements are important for mineral absorption.
Sodium Molybdate Dihydrate
In humans, molybdenum is known to function as a cofactor for four enzymes: Sulfite oxidase catalyzes the transformation of sulfite to sulfate, a reaction that is necessary for the metabolism of sulfur-containing amino acids (methionine and cysteine). In humans, molybdenum is known to function as a cofactor for four enzymes: Sulfite oxidase catalyzes the transformation of sulfite to sulfate, a reaction that is necessary for the metabolism of sulfur-containing amino acids (methionine and cysteine).
Nickel Sulphate
Nickel plays a role in the circulation of some proteins and contributes to the production of hormones, lipids, and cell membranes. Nickel is also used to break down glucose for energy. Nickel serve as a cofactor or structural component of specific metalloenzymes of various functions, including hydrolysis and redox reactions and gene expression. Also serve as a cofactor facilitating ferric iron absorption or metabolism. Nickel is necessary for the biosynthesis of the hydrogenase, carbon monoxide dehydrogenase, and of factor F-430. Nickel is a constituent part of all organs of vertebrates. Small amounts of nickel are found in DNA and RNA. Nickel therefore performs a vital function in metabolism and it is an essential element.
Sodium Borate
Studies with humans indicate that about 90 percent of boron is absorbed in the normal intake range. Most dietary boron is hydrolysed within the gut to yield B(OH)3 which, as a neutral compound, is easily absorbed. Boron chemistry suggests it is transported in the blood as B(OH)3. Specifically, because boron forms labile complexes in aqueous solution, transport is probably as free boric acid rather than a complex. The blood boron concentration is dependent on dietary intake as primarily shown by animal studies.
Benfotiamine
Thiamine is absorbed from the gastro-intestinal tract and is widely distributed to most body tissues. Amounts in excess of the body's requirements are not stored but excreted in the urine as unchanged thiamine or its metabolites.
Niacinamide
Nicotinic acid is absorbed from the gastro-intestinal tract, is widely distributed in the body tissues and has a short half-life.
Copper
Copper is absorbed from the gastro-intestinal tract and its major route of excretion is in the bile.
Manganese Sulphate
Manganese salts are poorly absorbed.
Choline Bitartrate
Very little information is available on its function and metabolism.
Lycopene
Lycopene absorption occurs via passive diffusion or facilitated by scavenger receptor class B type 1 (SR-B1) in enterocytes, potentially alongside other carotenoids. Partial cleavage by enzymes like Beta-Carotene Oxygenase 1 (BCO1) and Beta-Carotene Oxygenase 2 (BCO2) in enterocytes may occur. Transport involves packaging into chylomicrons, then release into the lymph and portal circulation. Lycopene primarily associates with LDL and is distributed to various organs, notably accumulating in the liver but also present in adipose tissue, adrenal glands, testes, ovaries, kidneys, lungs, skin, and the prostate. Lycopene and its metabolites are primarily eliminated from the body through fecal excretion, a smaller portion may be excreted via urine.
6.0 Nonclinical properties
6.1 Animal toxicology or Pharmacology
There are no pre-clinical data of relevance to the prescriber which are additional to that already included in other sections of the prescribing information.
7.0 Description
Bevon capsules contain a comprehensive formula of vitamins, minerals and antioxidants specially designed to support health and well-being in adults by unlocking energy and strengthening immunity. Most vitamins, minerals and trace elements are not produced by human body and hence are dependent on dietary supply of these nutrients. Since vitamins, minerals and trace elements are involved in many metabolic processes in the body, an adequate supply of these vital substances contribute to physical and mental well-being.
8.0 Pharmaceutical particulars
8.1 Incompatibilities
No major incompatibilities are known.
8.2 Shelf life
24 Months
8.3 Packaging information
A blister strip of 15 capsules.
8.4 Storage and handling instructions
Store in a cool & dry place. Protect from light.
Keep out of reach of children.
9.0 Patient counselling information
Do not take Bevon Capsules:
- if you are allergic (hypersensitive) to any of the ingredients of Bevon Capsules
- if you suffer from hypercalcaemia (high level of calcium in the blood)
- Do not give Bevon Capsules to children aged under 12.
Take special care with Bevon Capsules
Before you are given Bevon Capsules tell your doctor, dietician or pharmacist if:
- you are pregnant or thinking of becoming pregnant
- you are a smoker
If any of the above applies to you, or if you are not sure, speak to your doctor or pharmacist before taking Bevon Capsules.
Taking other medicines
Tell your doctor if you are taking or have recently taken/used any of the following medicines as they may interfere with Bevon Capsules:
- Phenytoin (used to treat epilepsy)
- Tetracycline antibiotics (used to treat infections) such as doxycycline and minocycline.
Please tell your doctor if you are taking or have recently taken/used any other medicines including other vitamin or mineral products medicines obtained without a prescription.
12.0 Date of revision
06/10/2021
About leaflet
Read all of this leaflet carefully before you start taking this medicine because it contains important information for you.
- Keep this leaflet. You may need to read it again.
- Ask your pharmacist if you need more information or advice
- You must contact a doctor if your symptoms worsen or do not improve
- If you get any side effects, talk to your doctor or pharmacist. This includes any possible side effects not listed in this leaflet. See section 4.
What is in this leaflet
1. What Bevon is and what it is used for
2. What you need to know before you take Bevon capsule
3. How to take Bevon capsule
4. Possible side effects
5. How to store Bevon capsule
6. Contents of the pack and other information
1. What Bevon capsule is and what it is used for
Bevon Capsules are a multivitamin, multi-mineral and anti-oxidant supplement. They contain a combination of 18 essential vitamins, minerals and trace elements. The human body requires a wide variety of vitamins, minerals and trace elements to perform crucial daily tasks such as releasing energy from food and repairing cell damage. During certain illnesses, your body either cannot get or cannot efficiently use all of the vitamins, minerals and trace elements it needs. Your doctor, dietician or pharmacist will give you Bevon Capsules if your diet has not provided you with enough vitamins, minerals and trace elements. Each capsule contains the following 18 essential vitamins, minerals and trace elements, each of which plays a vital role in the efficient daily maintenance of many body processes.
Each soft gelatin capsule contains:
Pyridoxine Hydrochloride IP 1.5 mg
Niacinamide IP 15 mg
Cyanocobalamin IP 0.5 mcg
Folic Acid IP 300 mcg
Choline Bitartrate USP 10 mg
Biotin IP 30 mcg
Betacarotene (30% Dispersion) USP 5 mg
Nickel Sulphate
equivalent to Elemental Nickel 15 mcg
Zinc Sulphate Monohydrate IP
equivalent to Elemental Zinc 7.5 mg
Sodium Selenite Pentahydrate BP
equivalent to Elemental Selenium 30 mcg
Copper Sulphate Pentahydrate BP
equivalent to Elemental Copper 2.5 mg
Chromium Picolinate IP
equivalent to Elemental Chromium 65 mcg
Manganese Sulphate USP
equivalent to Elemental Manganese 1.4 mg
Sodium Molybdate Dihydrate BP
equivalent to Elemental Molybdenum 25 mcg
Benfotiamine 2 mg
Sodium Borate BP
equivalent to Elemental Boron 150 mcg
Dibasic Calcium Phosphate IP
equivalent to Elemental Phosphorous 125 mg
Lycopene Preparations (10%) USP 5 mg
Excipients q.s.
In wheat germ oil virgin & flaxseed oil base.
Approved colours used in the capsule shell.
The functions of the vitamins found in Bevon capsule are:
| Vitamin A (β-Carotene) | Is essential for growth, maintenance of skin and mucous membranes such as the linings of the mouth, nose, lungs, digestive system, colon and for vision, particularly at night |
| Vitamin B6 (Pyridoxine) | Vitamin B6 helps protein metabolism, along with the maintenance of the nervous and immune systems |
| Vitamin B12 | Vitamin B12 is often called the 'red vitamin' because it is required for regulating blood cells |
| Biotin | Biotin is needed for normal growth and development of the skin and hair, the maintenance of a healthy nervous system and the healthy functioning of bone marrow |
| Niacinamide | Niacinamide (also known as vitamin B3) is essential for a healthy nervous system |
| Benfothiamne | Thiamine (Vitamin B1) is involved in the proper functioning of the heart muscles and for the release of energy from protein, fat and carbohydrate, needed for growth, normal appetite and digestion. Thiamin has also been shown to play a vital role in the normal functioning of the nervous system |
| Folic acid | Folic acid is required to regulate the growth of cells including red blood cells and protein synthesis |
The main functions of the minerals and trace elements are:
| Zinc | Zinc is required for growth and cell function, bone metabolism, taste, insulin production and the body’s immune system which fights infection. |
| Manganese | Manganese helps the body to utilize calcium and potassium and maintain the structure of cells. |
| Selenium | Selenium helps to protect the cells and lipids from free radical damage. |
| Chromium | Helps the body to use glucose by its action on insulin |
| Molybdenum | Is involved in the enzyme processes for protein metabolism. |
| Copper | Is required for growth and forms part of enzymes involved in blood and bone formation |
| Choline | Choline is a precursor to the neurotransmitter acetylcholine, participate in signal transduction, an essential process for cell growth, regulation and function. |
| Calcium Phosphate | Calcium is necessary for the formation of bones and teeth and plays a vital role in cell function, muscle contraction and in the nervous system. Phosphorus is necessary for the formation of bones and has an important role in many varied chemical reactions in the body |
| Sodium Borate | increase muscle mass; increase muscle strength; maintain bone density; improve calcium absorption and decrease body fat |
| Nickel | Nickel plays a role in the circulation of some proteins and contributes to the production of hormones, lipids, and cell membranes |
| Lycopene | Its potent antioxidant and anti-inflammatory effects may help protect against heart disease, skin disease, reproductive system diseases, certain types of cancer, and high blood sugar. It also aids in improving liver and bone health. |
2. What you need to know before you take Bevon capsule
- Do not take Bevon capsule if:
- Hypersensitivity to the active substance or to any of the excipients listed in the formulation.
- Whilst taking Bevon capsule, both protein and energy are also required to provide complete nutrition in the daily diet. No other vitamins, minerals or supplements with or without vitamin A should be taken with this preparation except under medical supervision.
- Evidence from Randomised Control Trials suggests that high doses (20-30 mg/day) β-carotene intake may increase the risk of lung cancer in current smokers and those previously exposed to asbestos. This high-risk population should consider the potential risks and benefits of Bevon capsule, which contain 5mg of β-carotene per recommended daily dose, before use.
- if you suffer from hypercalcaemia (high level of calcium in the blood)
Take special care with Bevon Capsule
Before you are given Bevon Capsules tell your doctor, dietician or pharmacist if:
- you are pregnant or thinking of becoming pregnant
- you are a smoker
- you have an asbestos related illness such as asbestosis
Do not take this medicine if any of the above apply to you. If you are not sure, talk to your doctor or pharmacist before taking Bevon capsule.
Pregnancy and breast-feeding
Bevon capsule contain vitamin A, check with your doctor, dietician or pharmacist for advice before taking this medicine during pregnancy.
Check with your doctor or pharmacist for advice before taking this medicine whilst breast-feeding
Other medicines and Bevon capsule
Tell your doctor if you are taking or have recently taken/used any of the following medicines as they may interfere with Bevon Capsules:
- Phenytoin (used to treat epilepsy)
- Tetracycline antibiotics (used to treat infections) such as doxycycline and minocycline.
Please tell your doctor if you are taking or have recently taken/used any other medicines including other vitamin or mineral products medicines obtained without a prescription. Tell your doctor if you are taking or have recently taken any other medicines.
3. How to take Bevon capsule
Adults and Elderly:
One capsule per day or as prescribed by the doctor. The capsules should be swallowed whole with a glass of water.
In Children
Do not give Bevon Capsules to children aged under 12
Capsule should be swallowed whole & not to be opened, chewed or crushed.
If you take more Bevon capsule than you should
If you (or someone else) accidentally take too many tablets, you should tell your doctor at once or contact the nearest accident and emergency department. Show any left-over medicines or the empty packet to the doctor
If you forget to take Bevon capsule
Do not worry. If you forget to take a dose, take it as soon as possible, unless it is almost time to take the next dose (within 1-2 hours). Do not take a double dose. Then go on as before.
4. Possible side effects
Like all medicines, Bevon capsule can cause side effects, although not everybody gets them.
Bevon capsule may cause allergic reactions (such as rash), and problems related to your stomach and intestines (such as feeling or being sick and stomach pains).
Reporting of side effects
- If you get any side effects, talk to your doctor. This includes any possible side effects not listed in this leaflet. You can also report side effects directly: Website: www.zuventus.com and click the tab “Safety Reporting” located on the top of the home page.
- By reporting side effects, you can help provide more information on the safety of this medicine.
5. How to store Bevon capsule
Keep out of the reach and sight of children.
Do not take Bevon Capsules after the expiry date which is stated on the carton. The expiry date refers to the last day of that month after EXP.
Store in cool and dry place. Keep the blister in the outer carton in order to protect from light.
Medicines should not be disposed of via wastewater or household waste. Ask your pharmacist on how to dispose of medicines no longer required. These measures will help protect the environment.
6. Contents of the pack and other information
What Bevon capsule contains.
Each soft gelatin capsule contains: Pyridoxine Hydrochloride, Niacinamide, Cyanocobalamin Folic Acid, Choline Bitartrate, Biotin, Beta-carotene Nickel, Zinc, Selenium, Copper Chromium. Manganese, Molybdenum, Benfotiamine, Boron, Dibasic Calcium Phosphate, Lycopene
Excipients q.s. In wheat germ oil virgin & flaxseed oil base
For More Information About This Product
Afpin Cl
Afpin Cl
COMPOSITION: Each serving per veg capsule contains: % RDA as per ICMR: Curcuma longa rhizome extract (as CurQlife NLT 10%) 400 mg, Boswelia Serrata extract (as Aflapin NLT 20%) 50 mg.
INDICATIONS: Treatment of patients with mild to moderate osteoarthritis.
ADVERSE EFFECTS: Nausea, headache, acidity, diarrhoea, rash, yellow stool, an increase in serum alkaline phosphatase and lactate dehydrogenase.
CONTRAINDICATION: Hypersensitivity to the active substance or to any of the excipients listed in the formulation.
PRECAUTIONS: Do not exceed the stated recommended daily dose, keep out of reach of children.
DOSAGE AND ADMINISTRATION: 1 capsule twice daily or as directed by a healthcare professional.